Download

1 / 37
410 likes | 709 Views
Human herpesviruses. Three subfamilies (genome structure, tissue tropism, cytopathologic effect, site of latent infection) Alphaherpesvirinae: Human herpesvirus 1 Herpes simplex type 1 HSV-1 Human herpesvirus 2 Herpes simplex type 2 HSV-2 Human herpesvirus 3 Varicella-zoster virus VZV

E N D
Human herpesviruses • Three subfamilies (genome structure, tissue tropism, cytopathologic effect, site of latent infection) • Alphaherpesvirinae: Human herpesvirus 1 Herpes simplex type 1 HSV-1 Human herpesvirus 2 Herpes simplex type 2 HSV-2 Human herpesvirus 3 Varicella-zoster virus VZV • Gammaherpesvirinae Human herpesvirus 4 Epstein-Barr virus EBV Oncogenic Human herpesvirus 8 Kaposi’s sarcoma related virus HHV-8 Oncogenic • Betaherpesvirinae Human herpesvirus 5 Cytomegalovirus CMV Congenital inf Human herpesvirus 6Herpes lymphotropic virus HHV-6 Human herpesvirus 7 Human herpesvirus 7 HHV-7
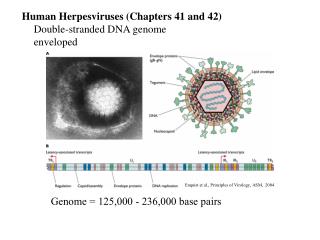
Human herpesviruses • Large, enveloped double stranded DNA viruses • Icosahedral capsid • Sensitive to acid, solvents, detergents and drying
Human herpesviruses They have common: • Virion morphology • Basic mode of replication • Capacity to establish latent and recurrent infections, in case of EBV immortalizing infections • Ubiquitous • Usually cause benign disease especially in children • In immunosuppressed people they cause significant morbidity and mortality
Human herpesviruses -DNA polymerase: -viral DNA replication -good target for antiviral drugs. -DNA replication and assembly:nucleus -buds from nuclear membrane, released by exocytosis and cell lysis. -lytic,persistant, latent, for EBV immortalizing infections
Herpes simplex virus • Two types: HSV-1 and HSV-2 • HSV can infect most types of human cells and even cells of other species. • Lytic infection of fibroblasts and epitelial cells but latent infection of neurons • The primary target cell: mucoepitelial cells • Site of latency: neurons
Herpes simplex virus • Means of spread: HSV-1 close contact, HSV-2 close contact+sexual transmission! • Generally cause infection at the site of infection • HSV-1: infections above the waist • HSV-2: infections below the waist • Growth characteristics are different • HSV-2 :more potential for viremia
Herpes simplex virus • Disease initiates by direct contact, depends on the infected tissue (oral, brain, genital) • Direct cytopathologic effect • Lytic infections of most cells, latent infection of neurons(hides from immune response) • Cell to cell spread-syncytia(avoids antibody) • Cowdry type A acidophilic intranuclear inclusion bodies
Herpes simplex virus • Initiates infection through mucosal membranes or breaks in the skin • Virus replicates in the cells at the base of the lession and infects the innervating neurons • Travels by retrograde transport to the ganglion( trigeminal ganglion for oral HSV, sacral ganglia for genital HSV)
Herpes simplex virus • Then turns to initial site of infection • May be inapparent or vesicular( vesicle fluid contains infectious virons) • Tissue damage: viral pathology+immunopathology • Heals without a scar • Latent infection occurs in neurons
Herpes simplex virus • Recurrence: stress, trauma, fever, sunlight) • The virus travels back down the nerve causing lessions at the dermatome • Recurrences are less severe and more localized
HSV-1 is common • 90% have antibody by 2 years of age • HSV-2 occurs later in life with sexual activity • Physicians,nurses,dentists at risk for infection of fingers (herpetic whitlow) • Immunocompromised people and neonates at risk of disseminated, life-threateneing disease.
Laboratory diagnosis • Cytology and histology: Tzanck smear(scraping of the base of a lesion), Papanicolaou smear or biopsy specimen • Cytopathic effects: syncytia, ballooning of cytoplasm, Cowdry A intranuclear inclusions • Direct antigen detection: immunofluorescence method or immunoperoxidase method • DNA :in situ hybridization or PCR in tissue or vesicle fluid
Laboratory diagnosis • Virus isolation: not routine now • Serology:primary infection, type specific antibody by ELISA (differentiates HSV-1 and HSV-2)
Varicella-Zoster • Chickenpox(varicella) • With recurrence :herpes zoster-shingles:zona • Primary target cell: mucoepitelial cell • Site of latency: neuron • Means of spread: respiratory and close contact • Viremia occurs after local replication :skin lessions over the entire body
Varicella-Zoster • Primary VZV infection: mucosa of respiratory tract • Viremia • Reticuloendotelial system,liver,spleen • 11-13 days later secondary viremia • Virus is spread through the body and skin=rash+fever+systemic symptoms
Varicella-Zoster • Latent in dorsal root or cranial nerve ganglia after primary infection • Reactivates in older adults and in patients with impaired immunity. • On reactivation : a vezicular rash along the entire dermatome • Children and leukemia: VZV more serious and more disseminated disease
Varicella-Zoster • Extremely communicable • Rates of infection exceeds 90% among household contact • Contagious before and during symptoms. • HZ develops in 10-20% of people infected with VZV and contains viable virus.
Varicella-Zoster • Laboratory diagnosis: • Cytology • Virus isolation: difficult • NAT • Serology • Treatment: • ACV,famciclovir and valacyclovir • Prophylaxis: VZIG:varicella-zoster immunoglobulin:immunosuppressed patients • A live attenuated vaccine(Oka strain)
Epstein-Barr Virus • Heterophile antibody-positive infectious mononucleosis • Chronic disease • Associated with endemic Burkitt’s lymphoma, Hodgkin’s disease, nasopharyngeal carcinoma, B-cell lymphomas in patients with acquired or congenital immunodeficiencies. • Hairy oral leukoplakia • Mitogen for B cells and immortalizes them
Epstein-Barr Virus Gammaherpesvirinae: Primary target cell: B cells and epitelial cells Site of latency: B cell Means of spread: saliva (kissing disease) Limited host range and tissue tropism: receptor for C3d component of the complement system (CR2 or CD21) which is expressed on B cells of humans and some epitelial cells of oro- and nasopharynx.
EBV-associated neoplasms • Geographic distribution • Co-factor? • Endemic Burkett’s lymphoma: Africa:malaria • Nasopharyngeal carcinoma: China
Laboratory diagnosis • Heterophile antibody: results from nonspecific activation of B cells by EBV • IgM antibody recognizes Paul-Bunnell antigen on sheep, horse and bovine erythrocytes not on guinea pig kidney cells • Detected at the end of first week , lasts for several months • Monotest, ELISA: specific antibodies • VCA-IgM, antibody to early antigen (EA): recent infection • VCA-IgG, EBNA: previous infection • PCR
Cytomegalovirus(CMV) • Betaherpesvirnae: lymphotropic • Primary target cell: monocyte, lymphocte, epitelial cell • Site of latency: monocyte, lymphocyte and? • Means of spread: close contact, transfusions, tissue transplant and congenital
Clinical findings • Predominant presentation: asymptomatic • Neonates: deafness, mental retardation • Immunosuppressed patients: disseminated dissease, severe disease (pneumonia, retinitis, colitis, esophagitis)
Congenital infection • An important cause of congenital disease • Serious birth defects is high if primary infection occurs during pregnancy • Microcephaly, intracerebral calcification,hepatosplenomegaly,rash(cytomegalic inclusion disease), unilateral or bilateral hearing loss, mental retardation • CMV in the urine in the first week (culture,PCR)
Laboratory tests • Cytology and histology: ‘OWL’s eye’ inclusion body basophilic intranuclear:Urine not so sensitive • Antigen in peripheral leucocytes • DNA by PCR • Cell culture: Human diploid fibroblasts • Serology: primary infection(IgM by ELISA)
Human herpesvirus 6 • Betaherpesvirinae • Lymphotropic , ubiquitous • Primary target cell: T cells and ? • Site of latency: T cells and ? • Means of spread: Respiratory, close contact • Exanthema subitum: roseola • A mononucleosis syndrome and lympadenopathy
Human herpesvirus 8 • HHV-8 DNA sequences were discovered by PCR in biopsy specimens of • Kaposi’s sarcoma (characteristic opportunistic diseases associated with AIDS) • Primary effusion lymphoma (rare type of B-cell lymphoma) • Multicentric Castleman’s disease
Human herpesvirus 8 • Kaposi’s sarcoma-related virus • Primary target cell: Lymphocyte and other cells • Site of latency:? • Means of spread: close contact, sexual, saliva? • Limited to certain geographic areas (Italy, Greece, Africa) and AIDS
Human herpesvirus 8 • Laboratory diagnosis: • Serology: specific antibodies:IFA IgG,IgM • HHV-8 DNA by PCR
Antivirals Herpes Simplex 1 and 2 Acyclovir Penciclovir Valacyclovir Famciclovir Adenosine arabinoside (ara-A) Trifluridine
Antivirals Varicella-Zoster Virus Acyclovir Famciclovir Valacyclovir Varicella-zoster immune globulin (VZIG) Zoster immune plasma Live vaccine Epstein-Barr Virus None
Antivirals Cytomegalovirus Ganciclovir* Valganciclovir* Iododeoxyuridine Foscarnet* Trifluridine Cidofovir*
Herpesvirus simiae(B virus) • Asian monkeys • Bites, saliva • Encephalopathy in humans • fatal