Download
1 / 70
790 likes | 1.68k Views
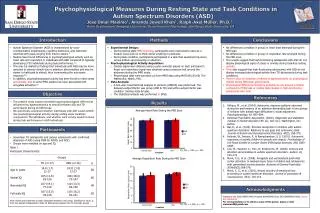
Psychophysiological Methods. Electrodermal Measurement. Galvanic skin response as indicative of the sympathetic branch of the autonomic nervous system Sweat glands provide a shunt between skin and deeper tissues Measures indicative of arousal, stress-strain, and emotion

E N D
Electrodermal Measurement • Galvanic skin response as indicative of the sympathetic branch of the autonomic nervous system • Sweat glands provide a shunt between skin and deeper tissues • Measures indicative of arousal, stress-strain, and emotion • Autonomic habituation provides a physiological measure of information processing capacity needed to complete a task • Used as measure of workload, mental strain, and emotional strain.
Procedure • Sampling across various locations of the body • Typically 3-4 cm distance between electrodes sampling dc current using a bioampifier • Sampling at 20hz sufficient to calculate Skin Conductive Response (SCR) • Amplitude, rise time and recovery time are measured • May be used to determine tonic Electrodermal Activity (EDA) to measure readiness for action
Three-Arousal Method of Measurement for the use of Psychophysiology in Ergonomics
Easy to measure and interpret the physiological signal Pure measure of the sympathetic branch of the ANS Sensitivity to workload and emotional strain Somewhat difficult to record Prone to artifacts in non-laboratory settings Indiscriminately sensitive to any ANS activity Several months of lab training to be able to use plus training for use in an ambulatory setting Advantages/Disadvantages
Short term reliability (within days) is fairly good (.80 to .90) Longer term reliability is more limited (.60) Tonic EDA more reliable than SCL (test-retest correlations of .76 and .61 at one year) Validity at or above .90 for EDA-Emotional strength in LAB setting No similar data for applied settings Validity based more on strength of emotion related to strain than physical relationship Heart rate and BP are yield better validity than EDA (.68 to .86) Reliability/Validity
Electromyography • Studies muscle function using electrical analysis of signals emanating at muscle contraction • Motor activity • Anterior horn of the spinal cord, transmitted via alpha motor neurons to muscle • Each muscle fiber consists of multiple chains of contractile sarcomeres (actin-myosin-filaments) • These filaments create muscle contraction • Motor unit chemically activates the muscle fibers connected as myoneural junction is depolarized (amplitude of about 100mV with a 2-14msec duration • Muscle action potential causes sarcomeres to contract • Electrodes in tissue or skin can measure these action potentials (electrolytic response)
EMG (continued) • Muscle force defined by motor units activated • EMG forms a quasi-randomly shaped spikes of amplitude and duration but no identifiable sequence • Correlation between number and intensity of generation of amplitude spikes and muscle contraction force • Remember, doesn’t measure force, joint position but rather voltage associated with local muscle recruitment
Use of EMG in the Workplace • Used for workplace and tool design • Muscle load (static and dynamic) • Local muscle fatigue due to overload • Muscle timing and coordination • Motor-unit recruitment • EMGs complemented by use of measures of external load, body posture, joint measurement • EMGs can be performed with needle electrodes inserted into muscle or surface electrodes
Procedure • Placement of electrodes or needles in muscles, signal passed to preamplifier, processed with band-pass filters for frequencies related to muscular activity • Select muscles related to action (may depend on how specific you want to be – measuring potential between muscle and ground • Amplify, filter and store results • Signal Processing • Scaling
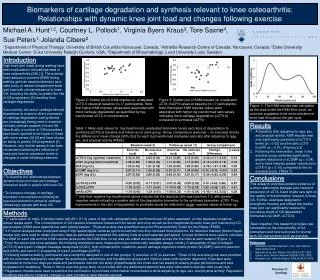
Correlation between feedback control and execution speed during learning an assembly task
Continuous and quantitative measured data High temporal resolution with marginal interference with task execution Allows detection of muscle fatigue at early stages providing objective measure Multi-channel EMG can identify muscular bottle-necks Surface EMG limited to muscles directly beneath area accessed by skin electrode Only feasible for single muscles in individuals not too obese Requires careful calibration, instrumentation, data manipulation, and interpretation Setup is fairly time consuming Interpretation requires data analysis and data integration Calibration lacks reliability Requires individual calibration, poor reliability Needle method more specific but invasive and quite painful EMG Advantages/Disadvantages
Heart Rate/Variability • Various Measures • Electrocardiogram (ECG) • Duration between heartbeats (HR) • Mean heart period or Interbeat Interval (IBI) • Heart Rate Variability (HRV) • Normal Rhythm • Cardiac Sinusoidal Mode • Modulated by innervations from the sympathetic and parasympathetic branches of the ANS • Heart Rate • Controlled by nuclei in the brain stem and guided by the hypothalamus and prefrontal cortical structures • Two control modes • Parasympathetic (Vagal) and Sypathetic output (Pores (1995)) • Mediation of bororeflex activity
HRV related to changes in autonomic control Vagal Gating NSR is vagally determined HRV and other cardiovascular variables modulated by baroreflex gain. General cardiac response found in mental-effort studies characterized by increased HR and BP and decreased HRV and BP variability at all frequencies Compatible with fight-flight reaction (lab studies, short-lasting tasks, challenging mental operations in working memory. Mid freq. band most sensitive to variation in mental effort due to decreased vagal activation and increased sympathetic activation. Use of ECG
Procedure • Three or 7 lead methods • Sampling and R-peak detection • Artifact detection and Correction • Spectral procedures • HR, IBI or Normalized Values? • Logarithmic Transformation
HR and HRV used as indicators of mental effort Higher invested effort, higher HR and lower HRV Complex relationship between HR with baroreflex BP control and autonomous nervous activity Most stable results only really found in lab settings Restrictions in sensitivity for artifacts in obtained IBI series and sensitivity for changes in respiration Artifact correction time consuming Newer technologies are mitigating some of these limitations Disadvantages
R and V of HR and HRV in short duration mental loading lab results usually high Doesn’t hold for practical settings Diagnostic validity and reliability debated Sensitivity of the measure not very high Difficult to distinguish levels of task load and related invested effort Requires multiple data collection sessions on single subject Validity affected by fight-flight mechanism versus compensatory mechanisms Reliability and Validity
Ambulatory EEG Methods • Sleepiness linked with accidents (Comair 5191) • Sleep loss, long time awake, work at circadian trough of physiological activation and alertness, monotony • Effects of drugs, alcohol, sedative, hypnotics, antihistamines all can have an effect. • Concept of sleepiness (various components) • Subjective • Behavioral • Physiological
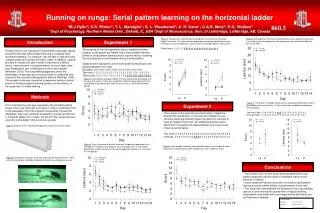
Methods • EEG – sum of electrical brain activity • Recorded at scalp or needle electrodes • When alertness falls, frequency of EEG falls and amplitude increases as more neurons synchronized to fire by the thalamus (rational behind EEG indicator of sleepiness) • Progression from Alpha (8-12Hz) to Theta (4-8Hz) to Delta (0-2Hz)
Procedure/Example • See text for in depth discussion of procedure for setup and use of EEG and EOG. • Example 12.1 shows EEG/EOG pattern in severe sleepiness performing a task and demonstrates beta activity, increased alpha activity, eye closure, slow eye rolling movements, and dozing off, reappearing beta activity, return of eye blinks
Application takes 15-30 minutes minimum for electrode placement Learning to setup takes 10-20 hours for reliable recording Scorring takes several months to learn Requires repeated quality checks Application/Training
No formal reliability established for ambulatory EEG methods Hard to define due to the definitions of the measures and the changing nature of the measure Several studies have defined validity between subjective sleepiness and sleepiness-impaired performance Purposeful interaction with the environment not possible when EEG dominated by alpha/theta and slow eye movements Reliability/Validity
Event Related Potentials (ERPs) • ERP – Transient series of voltage oscillations • Recorded from the scalp • Response to direct stimuli and responses • Often defined in terms of polarity and minimum latency with respect to discrete stimulus/response • Found to reflect perceptual, cognitive, motor processes • Useful to decompose processing requirements of complex tasks (Fabiani et al., 2000)
Procedure • Experimental paradigm design • Subject preparation • Preparation of ERP data for analysis • Component definition and pattern recognition • Data analysis
We possess understanding concerning functional significance of different ERP components Brain regions from which component generated are known ERPs can be obtained in absence of operator action/performance Motion artifacts Require discrete stimulus or response Substantial training required for recording, analysis, interpretation Advantages/Disadvantages
Depends on whether you want to learn the basics (2 months) or become knowledgeable about the basis of ERP signals (advanced degree) Application times from 15min for a few electrodes to 45min for large electrode array Training/Application Times
Validity of ERP components to specific cognitive constructs convincingly demonstrated Reliability established through extensive replications Split-half reliability high for P300 amplitude (.92) and latency (.83) Test-retest reliability over several days for P300 amplitude .83 and P300 latency .63 Reliability/Validity
EEG/MEG/fMRI • Neural activity generates currents outside the skull which can be monitored by their electrical and magnetic fields • Electroencephalogram (EEG) • Magnetoencephalogram (MEG) • Magnetic Resonance Imaging (MRI) • Functional MRI (fMRI) • Provide a basis for examining the neural substrate of specific cognitive processes
Movement-related brain activation Memory processes (encoding & retrieval) Visual perception, attention, & selection Auditory perception, attention & selection Language production and processing Perception of music Learning and brain plasticity with respect to cognitive functions Uses Neurosurgery Localization of epileptic foci based on specific brain areas spiking Estimation of the impact of certain lesions on higher neural functioning MEG preferred for temporal resolution; fMRI for spatial resolution; and maximum information when/where the two methods can be combined. Limited to patients without ferromagnetic inserts Research Areas amenable to MEG & fMRI
Requires use of superconducting quantum interference devices (SQUIDs) Exploit quantum mechanical “Josephson-effect” Modern MEG systems monitor signals from 150-300 SQUIDs spread equally over the head surface Variants of MEG sensors known as Gradiometers Spin tilt of protons aligned with strong magnetic field is pertubated by a brief electromagnetic pulse Protons emit burst of RF energy as they return to their initial aligned state Strength of signal with particular RF signature allows determination of proton density Helps define tissue characteristics at that location MEG/fMRI Mechanisms
Procedure (MEG) • Helmet like gantry placed over subject’s head • Coils fixed on head provide weak magnetic sources known as anatomical sites.
fMRI • Subject reclined on movable gantry, shifted into the bore of a magnet. • Structural scan • Repeated functional scans
Experimental Setup • During session, sequence of visual or auditory or other sensory stimuli is presented to the subject who has to process them according to a predefined task. • Often the same or similar stimuli are presented with slightly different task requirements • Differences between the BOLD responses in the different experimental conditions are evaluated to determine what brain regions are specifically activated by a particular task or sensory input
Event-locked epochs initially averaged separately for each subject, channel (sensor), task, or condition Epochs containing artifacts are rejected or correlated Grand average waveforms are scanned for components (peaks/troughs)(50-100msec) Time/amplitude measurements determined for each component, task, subject. Statistical analysis to ascertain significant differences which are localized to a region of the brain Various co registration techniques possible using nonlinear parameters, algorithms from chaos theory Analyzing continuous MEG data is based on chaos theory and beyond the scope of this class MEGData Analysis
Continuously recorded fMRI/BOLD data sorted according to different stimulus/task condition Any distortions are corrected by a processing algorithm. Those functional images showing significant differences in activation levels at the level of the individual voxels fMRI permits single subject statistical analysis due to better signal to noise ratios Comprehensive evaluation packages are available Statistical parametric mapping (SPM) package Also advanced applications that deconvolve temporally overlapping BOLD responses fMRI Data Analysis
Training • Predefined protocols performed by techs after two week training period • For more advanced/sophisticated applications, at least one full time engineer or physicist should be available (6 month training). • In clinical setting, support of a dedicated physician is required for data interpretation • Neuroscientists should have a sound background in experimental design as well as neurophysiological education. Specific training per investigations being conducted • Joint program between Emory and Georgia Tech provides degree and background in medical physics
Test Times • Experimental run may require about 1.5 hours with 15 minutes additional subject preparation
MEG Reliability/Validity • MEG • Artifacts can be minimized but not eliminated • Raw signals, an experienced rater can recognize these distortions • Potential artifacts depend on s/n • Avoid misinterpretation of waveform • Reasonable solutions possible but not foolproof. • Reliability and validity rely on user’s experience
fMRI Reliability/Validity • fMRI • Continuous maintenance should result in acceptable raw images • Artifacts due to discontinuities in magnetic susceptibility can lead to low structural distortions and signal loss • Easily detected but not readily corrected • Errors can be introduced to statistical analysis • Even with formal fMRI handling correct, erroneous conclusions may be drown from data obtained using inappropriate experimental designs • Reliability and validity of fMRI method also relies on user experience
Blood Pressure Measures • Strain affects mood and behavior • Performance and physiological effort have used strain analyses that are only psychological • Progress in ambulatory measurement has allowed assessment of behavioral, emotional and activational interaction with workload under real work conditions. • Low strain load has been used to investigate long term work (fatigue, boredom, vigilance) on health
Ambulatory BP • Developed clinically to measure physical work effects • Increased use for psychosocial work characteristics • Use of portable recorders for non-invasive recording