Download
1 / 91
920 likes | 1.34k Views
TREATING TOBACCO DEPENDENCE in SMOKERS with CO-OCCURRING SUBSTANCE ABUSE OR MENTAL HEALTH DISORDERS: SCIENTIFIC OVERVIEW. Judith J. Prochaska, PhD, MPH University of California, San Francisco. RATES of TOBACCO USE.

E N D
TREATING TOBACCO DEPENDENCE in SMOKERS with CO-OCCURRING SUBSTANCE ABUSE OR MENTAL HEALTH DISORDERS: SCIENTIFIC OVERVIEW Judith J. Prochaska, PhD, MPH University of California, San Francisco
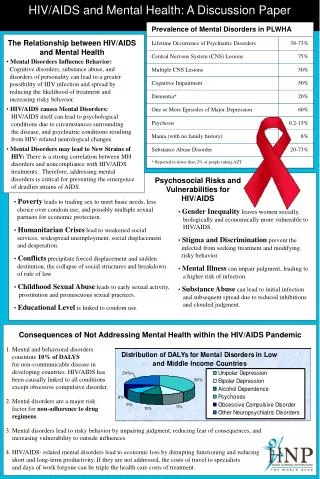
RATES of TOBACCO USE • Smoking rate among individuals with mental illness is 2 to 4 x’s that of the general population (Hughes, 1993; Poirier, 2002) • As many as 74% to 88% of individuals with addictive disorders smoke (Kalman, 1998), compared to 23% in the general population (CDC, 2002) • Account for 44% to 46% of cigarettes sold in the US (Lasser et al., 2000; Grant et al., 2004) 175 billion cigarettes $39 billion in annual sales
TRAJECTORIES OF USE • Earlier initiation of smoking • Heavier smoking • Greater nicotine dependence • Greater difficulty with quitting • Greater psychiatric, cognitive, & medical comorbidities • (e.g., Breslau et al., 1996; Burling et al., 1997; Novy et al., 2001; Richter et al., 2002; Saxon et al., 2003)
TRENDS in US ADULT SMOKING:1955–2004 Trends in cigarette smoking among persons aged 18 or older 20.9% of adults are current smokers Male Percent Female 22.9% 17.5% Graph provided by the Centers for Disease Control and Prevention. 1955 Current Population Survey; 1965–2004 NHIS. Estimates since 1992 include some-day smoking.
SMOKING by DIAGNOSIS 41.0% Overall National Comorbidity Survey 1991-1992 Source: Lasser et al., 2000 JAMA Active
SMOKING in CALIFORNIA Acton, Prochaska, Kaplan, Small & Hall. (2001) Addict Behav Prochaska, Gill, & Hall. (2004) Psychiatric Services
TOBACCO KILLS • Individuals with mental illness die, on average, 25 years prematurely (Colton & Manderscheid, 2006) • elevated risk for respiratory and cardiovascular diseases and cancer, compared to age-matched controls(Brown et al., 2000; Bruce et al., 1994; Dalton et al., 2002; Himelhoch et al., 2004; Lichtermann et al., 2001; Sokal, 2004). • Current tobacco use is predictive of future suicidal behavior, independent of depressive symptoms, prior suicidal acts, and other substance use(Breslau et al., 2005; Oquendo et al., 2004, Potkin et al., 2003).
TOBACCO & OTHER DRUG USE • Half of all deaths among individuals treated for alcohol dependence were tobacco-related (Hurt et al., 1996) • Death rate 4 times greater among long-term drug abusers who smoke cigarettes vs. those who do not (Hser et al., 1994) • Synergistic health consequences of tobacco and other drug use: 50% greater than the sum of each individually (Bien & Burge, 1990)
COMPARATIVE CAUSES of ANNUAL DEATHS in the UNITED STATES Individuals with mental illness or substance use disorders Number of Deaths (thousands) AIDS Obesity Alcohol Motor Homicide Drug Suicide Smoking Vehicle Induced Source: CDC
Cardiovascular disease Lung Disease Cancers Delayed healing & recovery after surgery Dyslipidemia Hypertension Macular degeneration Cataract Osteoporosis Periodontal disease Sexual dysfunction Reduced fertility in women Poor pregnancy outcomes SIDS, child asthma Mental Illness HEALTH RISKS ASSOCIATED with CHRONIC TOBACCO USE
COMPOUNDS in TOBACCO SMOKE An estimated 4,800 compounds in tobacco smoke Gases (~500 isolated) Particles (~3,500 isolated) • Carbon monoxide • Hydrogen cyanide • Ammonia • Benzene • Formaldehyde • Nicotine • Nitrosamines • Lead • Cadmium • Polonium-210 • Arsenic 11 proven human carcinogens
“LIGHT” CIGARETTES The difference between Marlboro and Marlboro Lights… • There are no true health benefits to light cigarettes. • Smokers compensate by either smoking more intensely (deeper inhalation) or by obstructing the vents. an extra row of ventilation holes Image courtesy of Mayo Clinic Nicotine Dependence Center - Research Program / Dr. Richard D. Hurt The Marlboro and Marlboro Lights logos are registered trademarks of Philip Morris USA.
“NO SAFE” LEVEL of SMOKING • Smoking even 1 to 4 cigarettes a day nearly triples the risk of death from heart disease • Smokers who consume fewer cigarettes can reduce their risk of lung cancer, but still face a much larger risk of premature death or disability compared with people who quit Source: Godtfredsen et al. (2005) JAMA, Bjartveit et al. (2005) Tobacco Control
QUITTING: HEALTH BENEFITS Time Since Quit Date Circulation improves, walking becomes easier Lung function increases up to 30% Lung cilia regain normal function Ability to clear lungs of mucus increases Coughing, fatigue, shortness of breath decrease 2 weeks to 3 months 1 to 9 months Excess risk of CHD decreases to half that of a continuing smoker 1 year Risk of stroke is reduced to that of people who have never smoked 5 years Lung cancer death rate drops to half that of a continuing smoker Risk of cancer of mouth, throat, esophagus, bladder, kidney, pancreas decrease 10 years Risk of CHD is similar to that of people who have never smoked after 15 years
YEARS of SURVIVAL GAINED RELATIVE to CONTINUED SMOKING Source: DH Taylor et al., 2002 American Journal of Public Health
WHY ADDRESS TOBACCO USE in PSYCHIATRIC POPULATIONS? Prevent Death Improve Health Optimize Psychiatric Medication Effects Reduce Isolation Patient $ Savings Tobacco Industry Profits Interest groups/politicians supported by Tobacco Industry Tax revenues
WHY do INDIVIDUALS with MENTAL ILLNESS SMOKE? Smoking in adolescence is associated with psychiatric disorders in adulthood, including: panic disorder, GAD and agoraphobia, depression and suicidal behavior, substance use disorders, and schizophrenia (Breslau et al., 2004; Weiser et al., 2004; Goodman, 2000; Johnson et al., 2000) MENTAL ILLNESS SMOKING Active psychiatric disorders are associated with daily smoking and progression to nicotine dependence (Breslau et al., 2004).
FACTORS ASSOCIATED with TOBACCO USE in those with MENTAL ILLNESS Biologic & Pharmacologic Genetic predisposition Alleviation of withdrawal Pleasure effects Weight control Psychological/Behavioral Conditioning effects Coping tool Social interactions Boredom Tobacco Use Systemic & Treatment Use of cigarettes for reinforcement Tobacco industry marketing efforts Failure to treat in psychiatry & addiction treatment settings
Dopamine Norepinephrine Acetylcholine Glutamate -Endorphin GABA Serotonin NEUROCHEMICAL and RELATED EFFECTS of NICOTINE N I C O T I N E Pleasure, reward Arousal, appetite suppression Arousal, cognitive enhancement Learning, memory enhancement Reduction of anxiety and tension Reduction of anxiety and tension Mood modulation, appetite suppr. Benowitz.Nicotine & Tobacco Research 1999;1(suppl):S159–S163.
DOPAMINE REWARD PATHWAY Prefrontal cortex Dopamine release Stimulation of nicotine receptors Nucleus accumbens Ventral tegmental area Nicotine enters brain Amygdala
Human smokers have increased nicotine receptors in the prefrontal cortex. High Low Nonsmoker Smoker CHRONIC ADMINISTRATION of NICOTINE: EFFECTS on the BRAIN Image courtesy of George Washington University / Dr. David C. Perry Perry et al. J Pharmacol Exp Ther 1999;289:1545–1552.
GENETIC EFFECTS on NICOTINE METABOLISM 4.4% 0.4% 9.8% Nornicotine Nicotine-1'- N-oxide Nicotine Nicotine Nicotine glucuronide CYP2A6 Aldehyde oxidase 4.2% ~80% Trans-3'- hydroxycotinine Trans-3'- hydroxycotinine Cotinine Cotinine 13.0% 33.6% Trans-3'- hydroxycotinine glucuronide Cotinine glucuronide 12.6% Norcotinine 7.4% Cotinine- N-oxide 2.0% Reprinted with permission, Benowitz et al., 1994. 2.4%
NICOTINE ADDICTION CYCLE Reprinted with permission. Benowitz. Med Clin N Am 1992;2:415–437.
NICOTINE WITHDRAWAL EFFECTS • Dysphoric or depressed mood • Insomnia and fatigue • Irritability/frustration/anger • Anxiety or nervousness • Difficulty concentrating • Impaired task performance • Increased appetite/weight gain • Restlessness and impatience • Cravings* Most symptoms peak 24–48 hr after quitting and subside within 2–4 weeks. American Psychiatric Association. (1994). DSM-IV. Hughes et al. (1991). Arch Gen Psychiatry 48:52–59. Hughes & Hatsukami. (1998). Tob Control 7:92–93. * Not considered a withdrawal symptom by DSM-IV criteria.
WHAT is ADDICTION? “Compulsive drug use, without medical purpose, in the face of negative consequences” Alan I. Leshner, Ph.D. Former Director, National Institute on Drug Abuse National Institutes of Health
PSYCHIATRISTS in PRACTICE(Himelhoch & Daumit, 2003) • 1992-96 Nat’l Ambulatory Medical Care Survey • 23% of psychiatric visits dropped from analysis because patient smoking status unknown • For patients identified as smokers (N=1610) • Cessation counseling offered at 12% of visits • Nicotine Dependence not diagnosed at any visit • NRT never prescribed
PSYCHIATRY RESIDENTS’ (N=105) ENGAGEMENT in the 5-As Nationally, only 50% of Adult Psychiatry Residency Programs provide training in treating nicotine dependence. Training duration is a median of 1-hour (Prochaska et al., 2006). Source: Prochaska, Fromont et al., 2005 Acad Psychiatry
ATTENTION to TOBACCO USE in ADDICTION TREATMENT • Absent from most addictions treatment settings • 223 addiction treatment programs in Canada: • 10% offered formal smoking cessation programs • 54% reported placing very little emphasis on smoking • 47% still allowed smoking indoors (Currie et al., 2003). • Reluctance to encourage smoking cessation for fear that sobriety may be compromised
BARRIERS to TREATING TOBACCO • Smoking not viewed as a clinical issue • Our clients aren’t interested in quitting • Our clients can’t quit • Our clients need to smoke to manage their psychiatric symptoms and/or sobriety • Lack of training among providers • Not enough time, money…
BARRIERS to TREATING TOBACCO • Smoking not viewed as a clinical issue • Our clients aren’t interested in quitting • Our clients can’t quit • Our clients need to smoke to manage their psychiatric symptoms and/or sobriety • Lack of training among providers • Not enough time, money…
Pub. 1951 SMOKING in PSYCHIATRY
Tobacco Documents Department of Health, Education, and Welfare National Institute of Mental Health Washington, DC August 4, 1980 I am writing to request a donation of cigarettes for long-term psychiatric patients…because of recent changes in the DHHS regulations, Saint Elizabeth Hospital can no longer purchase cigarettes for them. I am therefore requesting a donation of approximately 5,000 cigarettes a week (8 per day for each of the 100 patients without funds).
JCAHO DECISION JCAHO ultimately “yielded to massive pressure from mental patients and their families, relaxing a policy that called on hospitals to ban smoking.” An exception was made to allow continued smoking in psychiatric inpatient and substance use facilities for long-term patients.
LD 463 - An Act to Exempt Substance Abuse and Psychiatric Patients from the Prohibition against Smoking in Hospitals
DSM-IV TOBACCO USE DISORDERS Nicotine Dependence • Maladaptive pattern of use with significant impairment manifested by 3+ in 12-months: • Tolerance • Withdrawal • Use • Unsuccessful efforts to stop • Time investment • Loss of important activities • Continued use despite knowledge of physical or psychological problems Nicotine Withdrawal • Daily use of nicotine • Abrupt cessation/reduction followed within 24 hrs by 4+: • Depressed mood • Insomnia • Irritability • Anxiety • Difficulty concentrating • Decreased HR • Increased appetite • Clinically significant impairment • Not due to GMC The majority of smokers with mental illness meet criteria for DSM-IV nicotine dependence and withdrawal (Prochaska et al., 2004; 2006)
TOBACCO IMPACTS TREATMENT * Significant group difference in rates of against medical advice (AMA) hospital discharge (χ2 = 6.79, df = 2, p = .034), even after controlling for group differences. Prochaska, Gill, & Hall. (2004) Psychiatric Services
Caffeine Clozapine (Clozaril™) Fluvoxamine (Luvox™) Haloperidol (Haldol™) Olanzapine (Zyprexa™) Phenothiazines (Thorazine, Trilafon, Prolixin, etc.) Propanolol Tertiary TCAs / cyclobenzaprine (Flexaril™) Thiothixene (Navane™) Other medications: estradiol, mexiletene, naproxen, phenacetin, riluzole, ropinirole, tacrine, theophyline, verapamil, r-warfarin (less active), zolmitriptan PHARMACOKINETIC DRUG INTERACTIONS of SMOKING Drugs that may have a decreased effect due to induction of CYP1A2: (Zevin & Benowitz, 1999) Smoking cessation may reverse the effect.
WHY MENTAL HEALTH and ADDICTION TREATMENT PROVIDERS? • Often the clinician for whom contact is the most frequent and who knows the patient best • Able to combine psychopharmacological and behavioral/counseling treatment • Trained in substance abuse treatment • Able to identify and address any changes in mental health or other substance use during the quit attempt
BARRIERS to TREATING TOBACCO • Smoking not viewed as a clinical issue • Our clients aren’t interested in quitting • Our clients can’t quit • Our clients need to smoke to manage their psychiatric symptoms and/or sobriety • Lack of training among providers • Not enough time, money…
* No relationship between psychiatric symptom severity and readiness to quit STUDIES of PSYCHIATRIC PATIENTS’ READINESS to QUIT* Smokers with mental illness are just as ready to quit smoking as the general population of smokers.
INTEREST in TREATMENT • Stage-based tobacco treatment study in inpatient psychiatry – recruiting 82% of eligible smokers (Prochaska et al., in process) • Stage-based tobacco treatment study with depressed smokers – 32% entered Cessation Treatment component (Haug et al., 2005)
TIMING of TOBACCO TREATMENT • 44 - 80% of individuals in addictions treatment report interest in quitting their tobacco use • 17 - 41% report concern that quitting during addictions treatment may make it harder to stay sober(Asher et al., 2003; Irving et al., 1994; Stein & Anderson, 2003) • Questions of when and how best to intervene
BARRIERS to TREATING TOBACCO • Smoking not viewed as a clinical issue • Our clients aren’t interested in quitting • Our clients can’t quit • Our clients need to smoke to manage their psychiatric symptoms and/or sobriety • Lack of training among providers • Not enough time, money…
Sharon Hall, PhD, Janice Tsoh, PhD, Judith Prochaska, PhD, MPH, Stuart Eisendrath, MD, Joseph Rossi, PhD, Colleen Redding, PhD, Amy Rosen, PsyD, Marc Meisner, MD, Gary Humfleet, PhD, & Julie Gorecki, MA University of California, San Francisco Supported by NIDA #P50 DA09253 Am J Public Health 2006 TREATMENT of DEPRESSED PSYCHIATRIC OUTPATIENTS for CIGARETTE SMOKING
STUDY DESIGN • 322 depressed smokers recruited from four outpatient psychiatry clinics • Stepped Care Intervention • Stage-based expert system counseling • Nicotine patch • 6 session individual CBT counseling • Bupropion available • Brief Contact Control • Primary outcome: • 7 day PPA @ 12 & 18 months, CO verified