Download
1 / 1
20 likes | 261 Views
CQI Project : Quiet Hour Compliance University of Wisconsin-Madison School of Nursing Group 9: Elle Bowman, Lauren Falkenberg , Heidi Jung, Shane McQuade , Laura Pogatchnik, and Lori Tebrinke. OPPORTUNITY STATEMENT :. FLOW CHART: 7 STEP MEETING PROCESS. PDCA :.

E N D
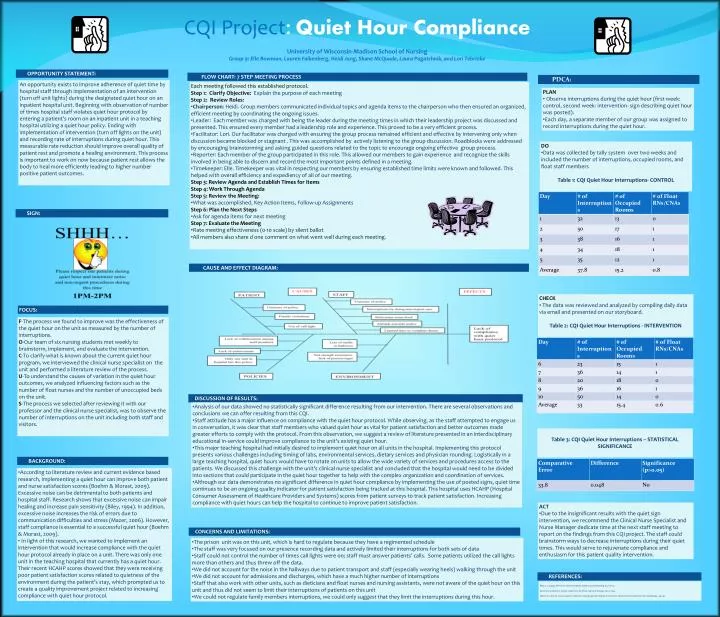
CQI Project: Quiet Hour Compliance University of Wisconsin-Madison School of Nursing Group 9: Elle Bowman, Lauren Falkenberg, Heidi Jung, Shane McQuade, Laura Pogatchnik, and Lori Tebrinke OPPORTUNITY STATEMENT: FLOW CHART: 7 STEP MEETING PROCESS PDCA: An opportunity exists to improve adherence of quiet time by hospital staff through implementation of an intervention (turn off unit lights) during the designated quiet hour on an inpatient hospital unit. Beginning with observation of number of times hospital staff violates quiet hour protocol by entering a patient’s room on an inpatient unit in a teaching hospital utilizing a quiet hour policy. Ending with implementation of intervention (turn off lights on the unit) and recording rate of interruptions during quiet hour. This measurable rate reduction should improve overall quality of patient rest and promote a healing environment. This process is important to work on now because patient rest allows the body to heal more efficiently leading to higher number positive patient outcomes. • Each meeting followed this established protocol. • Step 1: ClarifyObjective: Explain the purpose of each meeting • Step 2: Review Roles: • Chairperson: Heidi. Group members communicated individual topics and agenda items to the chairperson who then ensured an organized, efficient meeting by coordinating the ongoing issues. • Leader: Each member was charged with being the leader during the meeting times in which their leadership project was discussed and presented. This ensured every member had a leadership role and experience. This proved to be a very efficient process. • Facilitator: Lori. Our facilitator was charged with ensuring the group process remained efficient and effective by intervening only when discussion became blocked or stagnant . This was accomplished by actively listening to the group discussion. Roadblocks were addressed by encouraging brainstorming and asking guided questions related to the topic to encourage ongoing effective group process. • Reporter: Each member of the group participated in this role. This allowed our members to gain experience and recognize the skills involved in being able to discern and record the most important points defined in a meeting. • Timekeeper: Elle. Timekeeper was vital in respecting our members by ensuring established time limits were known and followed. This helped with overall efficiency and expediency of all of our meeting. • Step 3: Review Agenda and Establish Times for Items • Step 4: Work Through Agenda • Step 5: Review the Meeting: • What was accomplished, Key Action Items, Follow-up Assignments • Step 6: Plan the Next Steps • Ask for agenda items for next meeting • Step 7: Evaluate the Meeting • Rate meeting effectiveness (0-10 scale) by silent ballot • All members also share d one comment on what went well during each meeting. • PLAN • Observe interruptions during the quiet hour (first week: control, second week: intervention- sign describing quiet hour was posted). • Each day, a separate member of our group was assigned to record interruptions during the quiet hour. • DO • Data was collected by tally system over two weeks and included the number of interruptions, occupied rooms, and float staff members • Table 1: CQI Quiet Hour Interruptions- CONTROL SIGN: CAUSE AND EFFECT DIAGRAM: • CHECK • The data was reviewed and analyzed by compiling daily data via email and presented on our storyboard. • Table 2: CQI Quiet Hour Interruptions - INTERVENTION FOCUS: F-The process we found to improve was the effectiveness of the quiet hour on the unit as measured by the number of interruptions. O-Our team of six nursing students met weekly to brainstorm, implement, and evaluate the intervention. C-To clarify what is known about the current quiet hour program, we interviewed the clinical nurse specialist on the unitand performed a literature review of the process. U-To understand the causes of variation in the quiet hour outcomes, we analyzed influencing factors such as the number of float nurses and the number of unoccupied beds on the unit. S-The process we selected after reviewing it with our professor and the clinical nurse specialist, was to observe the number of interruptions on the unit including both staff and visitors. DISCUSSION OF RESULTS: • Analysis of our data showed no statistically significant difference resulting from our intervention. There are several observations and conclusions we can offer resulting from this CQI. • Staff attitude has a major influence on compliance with the quiet hour protocol. While observing, as the staff attempted to engage us in conversation, it was clear that staff members who valued quiet hour as vital for patient satisfaction and better outcomes made greater efforts to comply with the protocol. From this observation, we suggest a review of literature presented in an interdisciplinary educational in-service could improve compliance to the unit's existing quiet hour. • This major teaching hospital had initially desired to implement quiet hour on all units in the hospital. Implementing this protocol presents various challenges including timing of labs, environmental services, dietary services and physician rounding. Logistically in a large teaching hospital, quiet hours would have to rotate on units to allow the wide variety of services and procedures access to the patients. We discussed this challenge with the unit's clinical nurse specialist and concluded that the hospital would need to be divided into sections that could participate in the quiet hour together to help with the complex organization and coordination of services. • Although our data demonstrates no significant difference in quiet hour compliance by implementing the use of posted signs, quiet time continues to be an ongoing quality indicator for patient satisfaction being tracked at this hospital. This hospital uses HCAHP (Hospital Consumer Assessment of Healthcare Providers and Systems) scores from patient surveys to track patient satisfaction. Increasing compliance with quiet hours can help the hospital to continue to improve patient satisfaction. • Table 3: CQI Quiet Hour Interruptions – STATISTICAL SIGNIFICANCE BACKGROUND: • According to literature review and current evidence based research, implementing a quiet hour can improve both patient and nurse satisfaction scores (Boehm & Morast, 2009). Excessive noise can be detrimental to both patients and hospital staff. Research shows that excessive noise can impair healing and increase pain sensitivity (Biley, 1994). In addition, excessive noise increases the risk of errors due to communication difficulties and stress (Mazer, 2006). However, staff compliance is essential to a successful quiet hour (Boehm & Morast, 2009). • In light of this research, we wanted to implement an intervention that would increase compliance with the quiet hour protocol already in place on a unit. There was only one unit in the teaching hospital that currently has a quiet hour. Their recent HCAHP scores showed that they were receiving poor patient satisfaction scores related to quietness of the environment during the patient’s stay, which prompted us to create a quality improvement project related to increasing compliance with quiet hour protocol. • ACT • Due to the insignificant results with the quiet sign intervention, we recommend the Clinical Nurse Specialist and Nurse Manager dedicate time at the next staff meeting to report on the findings from this CQI project. The staff could brainstorm ways to decrease interruptions during their quiet times. This would serve to rejuvenate compliance and enthusiasm for this patient quality intervention. CONCERNS AND LIMITATIONS: • The prison unit was on this unit, which is hard to regulate because they have a regimented schedule • The staff was very focused on our presence recording data and actively limited their interruptions for both sets of data • Staff could not control the number of times call lights were on; staff must answer patients’ calls. Some patients utilized the call lights more than others and thus threw off the data. • We did not account for the noise in the hallways due to patient transport and staff (especially wearing heels) walking through the unit • We did not account for admissions and discharges, which have a much higher number of interruptions • Staff that also work with other units, such as dieticians and float nurses and nursing assistants, were not aware of the quiet hour on this unit and thus did not seem to limit their interruptions of patients on this unit • We could not regulate family members interruptions, we could only suggest that they limit the interruptions during this hour. REFERENCES: Biley, F. C. (1994). Effects of noise in hospitals. British Journal of Nursing, 3.3, 110-113. Boehm, H. & Morast, S. (2009). Quiet time. American Journal of Nursing, 109.11, 29-32. Mazer, S. E. (2006). Increase patient safety by creating a quieter hospital environment. Biomedical Instrumentation and Technology, 145-146.