Download
1 / 31
1.17k likes | 7.95k Views
Semen Analysis. Objective:. Physiology of semen formation Indication of semen analysis Macroscopic examinationof semen Microscopic examination Antibody testing in semen Reference ranges. Physiology of Seminal fluid .

E N D
Objective: • Physiology of semen formation • Indication of semen analysis • Macroscopic examinationof semen • Microscopic examination • Antibody testing in semen • Reference ranges
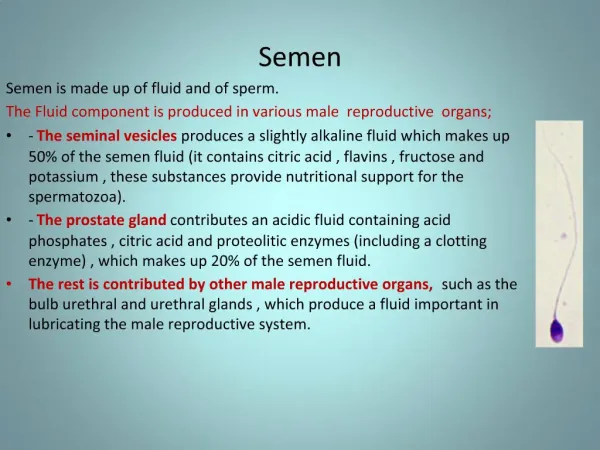
Physiology of Seminal fluid • Semen is grey opalescent fluid , which consists of suspension of spermatozoa in seminal plasma. • It is made up of the secretions of all accessoryglands of the male genital tract.
The Percentage contribution of Each of the Secretions in Seminal Fluid
Fructose: imp energy for sperms especially needed for sperms motility Prostaglandins: play a role in controlling sperm movement & sperm penetration of cervical mucus Fibrinogen-like substance : acted upon by enzyme vesiculase to induce clotting that occurs in semen The prostatic fluid pH =6.5 Enzymes: vesiculase Acid phosphatase
Bulbo-uretheral & uretheral glands The fluid rich in mucoprotein , so it lubricates the urethra Occasionally in the secretions contain antisperm antibodies( may be of importance in infertility cases)
During ejaculation , each of the components that make up semen may be discharged from the urethra in a sequence • The first part is made up of testicular component of semen followed by secretion of the prostate , lastly the secretion of the vesicles are expelled.
Indication of Semen Analysis • Assessment of fertility/infertility ( most common) • Determination the effectiveness of vasectomy • Determination of suitability of semen for artificial insemination • Follow up of fertility after cancer treatment by radio- or chemotherapy • Forensic purpose
Semen analysis • Specimens: • 2 samples should be collected for initial evaluation, • the interval between the two collections should not be less than 7 days or more than 3 weeks , • if the results of these assessments are markedly different , additional samples should be examined
Examination of Semen • Macroscopic Examination • Volume • Liquefaction time • Appearance • pH • Viscosity • Microscopic Examination • Sperm count • Sperm motility • Sperm viability • Sperm morphology • Agglutination • Antibodies coating of sperms • Biochemical Tests • Fructose test • Acid phosphatase
Volume : ( 2-6ml/ ejaculation) • Aspermia: total absence of ejaculation ( rare) • Hypospermia or oligospermia: the seminal fluid is < 2ml • Hyperspermia: volume > 10 ml • ( spermia denotes seminal fluid not spermatozoa)
Liquefaction time: • ( forms gel-like clot immediately after ejaculation) • a normal semen sample liquefies with 15 -60 mint . • ( prolongation must be recorded).
Appearance: • homogeneous , grey-opalescent appearance • The color is due to high content of protein &presence of > 60 million sperms/ml • May be less opaque if sperm concentration is very low • Dense white turbid in inflammation and high WBCs • Haematospermia :when red blood cells are present (blood) • Yellow in patient with jaundice (very bright yellow due to bilirubin) or taking some vitamins • Or contaminated with urine ( uriniferousodour)
pH : • between7.2-8.0 recorded in fresh semen by using pH paper . • A patient exceeding pH 8.0 may suggest acute disease of the seminal vesicles • Lowering of pH may be due chronic inflammatory of seminal vesicles • Or contamination with urine
Viscosity : • Normal viscosity is that which allows semen to be poured drop by drop out of the container. • In case of abnormal viscosity drop will form a thread more than 2 cm long • High viscosity : can interfere determination of sperm motility
Sperm Count: • Total number of sperms in an ejaculation. • It is 20 million/ml i.e. 60 million / ejac • It is obtained by multiplying the sperm concentration by the volume • Azoospermia: means no spermatocytes ( male sterility) • Oligozoospermia: < 20 million/ml (less than 50 million/ejaculation • Polyzoospermia : may reach 350millions/ejaculation
Sperm Count Decreased: vasectomy varicocele primary testicular failure (Klinefelters) secondary testicular failure congenital vas deferens obstruction endocrine causes (prolactinemia, low testosterone)
Assessment of sperm motility: • the motility of each spermatozoon is graded : • ‘a’ =rapid progressive motility • ‘b’= slow or sluggish motility • ‘c’= non progressive motility • ‘d’= immotility
Viability should be determined if the % of immotile spermatozoa exceeds 50 % Supravital stain: Eosin /Nigrosin Viable do not take up the stain
Normally the sperm count contains fewer than 20 % abnormal forms e.g. bitailed, short tailed , 2 heads …..etc.
Other cellular elements: • Leukocytes: • leukocytes predominantly neutrophils are present in most human ejaculate. • Normal <1x106 /ml or < 5/HPF • 5-20 WBC/HPF =increased • 20-40 WBCs/HPF =+ • >40 WBCs/ HPF = ++ • If increased leukospermia or pyospermiamay be associated with infection and poor sperm quality • When the number is increased, microbiological tests should be performed to investigate the presence of of infection in any of the accessory glands
Agglutination Reported when motile sperm stick to each other in a definite pattern. Head-head Tail-tail Head-tail Immunological cause of infertility
Biochemical Tests • Fructose Test: • It is secreted for sperm nutrition from seminal vesicle • Impairment of seminal vesicular secretion will result in reduced fructose secretion in semen and the motility of the sperms will be reduced. • Fructose disappears in cases of : • (a) absence of seminal vesicle; • (b) obstruction of ejaculatory duct; and • (c) inflammation of seminal vesicle. It is decreased in case of testosterone deficiency. So, fructose is used as fertility test.
Acid phosphatase: • Secreted from the prostate. • The test is used as: 1)A marker of prostatic functions; and 2)In forensic laboratories as a test for the presence of semen.
Testing for Antibody coating of spermatozoa • Sperms can induce immune response not only between species but also within one species and within an individuals • Sperm antibodies may : • Cause agglutination of sperm • Cause reduction in motility • Inhibit the ability of sperm to penetrate cervical mucus • Impede binding of the sperm to the oocyte • Antibodies may be IgA & IgG
Volume 2.0-6.0 ml pH 7.2-8.0 Color: greyish white Liquefaction: 15-60 min. Count >20 million/ml Total count > 40 million/ejaculate Motility: > 50 % motile( grades a+b) or > 25% with progressive motility ( grade a) within 60 minutes of ejaculaton Morphology > 30% normal form Viability > 75% viable WBC< 1million/ml RBC none