Download
1 / 26
260 likes | 597 Views
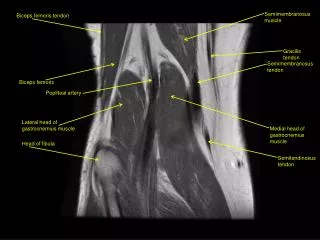
Rectus femoris transfer. 분당서울대학교병원 이승열. Rectus femoris muscle. Origin Anterior Inferior Iliac Spine and Ilium above toe acetabulum. Insertion Quadriceps tendon to base of patella and onto tibial tuberosity via the patellar tendon Nerve to muscle Femoral nerve (L2-L4).

E N D
Rectus femoris transfer 분당서울대학교병원 이승열
Rectus femoris muscle • Origin • Anterior Inferior Iliac Spine and Ilium above toe acetabulum
Insertion • Quadriceps tendon to base of patella and onto tibial tuberosity via the patellar tendon • Nerve to muscle • Femoral nerve (L2-L4)
One of m/c gait abnormality in patients with spastic CP • Typical finding • Decreased ROM of knee during swing phase • Foot clearance problem • Reduced gait velocity • Reduced step length
Rectus femoris transfer • Conventional treatment
Indication • Positive Duncan-Ely sign
Gait analysis Decreased knee flexion in swing Decreased and delayed peak knee flexion in sweing
Dynamic electromyography • Pathological increased activity of the rectus femoris muscle
Keep the rectus as a hip flexor • Convert the rectus into a knee flexor??? • Elimination of the rectus femoris activity
Study plan • Patients • 321 pts • Factors affecting the results of RFT • Age • Gender • Anatomical type • Functional scale (GMFCS level) • SEMLS concomitant with RFT
Long term results • LMM? • Gait analysis (knee sagittal motion) • GDI
Isokinetic muscle strength • Isometric muscle strength
Hip • Flexion/extension • Adduction/abduction • Knee • Flexion/extension • Ankle • Dorsiflexion/plantarflexion • Inversion/eversion