Download
1 / 19
200 likes | 749 Views
Penetrating Thoracic Injuries Andrew L. Singer January 18, 2005 Primary Survey Airway Breathing Circulation Anatomic Structures Chest Wall Thoracic Vertebrae and Cord Diaphragm Mediastinal Structures Heart Aorta Great Vessels Aerodigestive Tract Pulmonary Parenchyma Bony Thorax

E N D
Penetrating Thoracic Injuries Andrew L. Singer January 18, 2005
Primary Survey • Airway • Breathing • Circulation
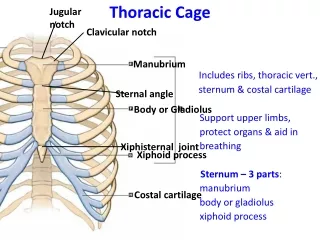
Anatomic Structures • Chest Wall • Thoracic Vertebrae and Cord • Diaphragm • Mediastinal Structures • Heart • Aorta • Great Vessels • Aerodigestive Tract • Pulmonary Parenchyma
Diaphragm • Muscular, dome-like structure • Separates abdomen from the thoracic cavity • Affixed to the lower border of the rib cage • Central and superior margin extends to the level of the 4th rib anteriorly and 6th rib posteriorly • Major muscle of respiration • Draws downward during inspiration • Moves upward during exhalation
Most injuries to the chest can be successfully managed without surgical intervention.
Hemothorax • Tube thoracostomy is adequate treatment in the majority of patients with traumatic hemothorax • The pressure of the pulmonary paranchymal circulation is low and is readily tamponaded with thoracostomy re-expansion • Thoracotomy for massive bleeding • >1500 mL initial output • >200 mL/h for 4 hours
Surgical Exploration The choice of position and surgical approach is dictated by the nature of the patient’s thoracic injuries, the certainty of diagnosis, and potential for associated injuries involving other body sites.
Anterolateral Thoracotomy • Aortic crossclamping • Emergent decompression of pericardial tamponade • Open cardiac massage • Allows access to abdomen and contralateral side (clamshell)
Median Sternotomy • Preferred Exposure to Heart and Aortic Arch and Great Vessels • Difficult Exposure to Lungs, Descending Aorta, Diaphragm and Esophagus
Posterolateral Thoracotomy • Makes access to contralateral side and abdomen nearly impossible • Provides optimal exposure to the contents of a particular hemithorax • Mid-esophageal injuries best approached from right side • Descending aorta from left • Repair of pulmonary vasculature and airway injuries
Additional Surgical Approaches • Subxiphoid pericardial window • Diagnostic and/or therapeutic laparoscopy to assess diaphragmatic injuries