Download
1 / 30
300 likes | 1.01k Views
Abbreviations. ACC: American College of Cardiology ACEI: angiotensin-converting enzyme inhibitor ACIP: Asymptomatic Cardiac Ischemia Pilot AHA: American Heart Association AV: arteriovenous CABG: coronary artery bypass grafting CAD: coronary artery disease CASS: Coronary Artery Surgery Study CHD: coronary heart disease CT: computed tomographyCVD: cardiovascular disease .

E N D
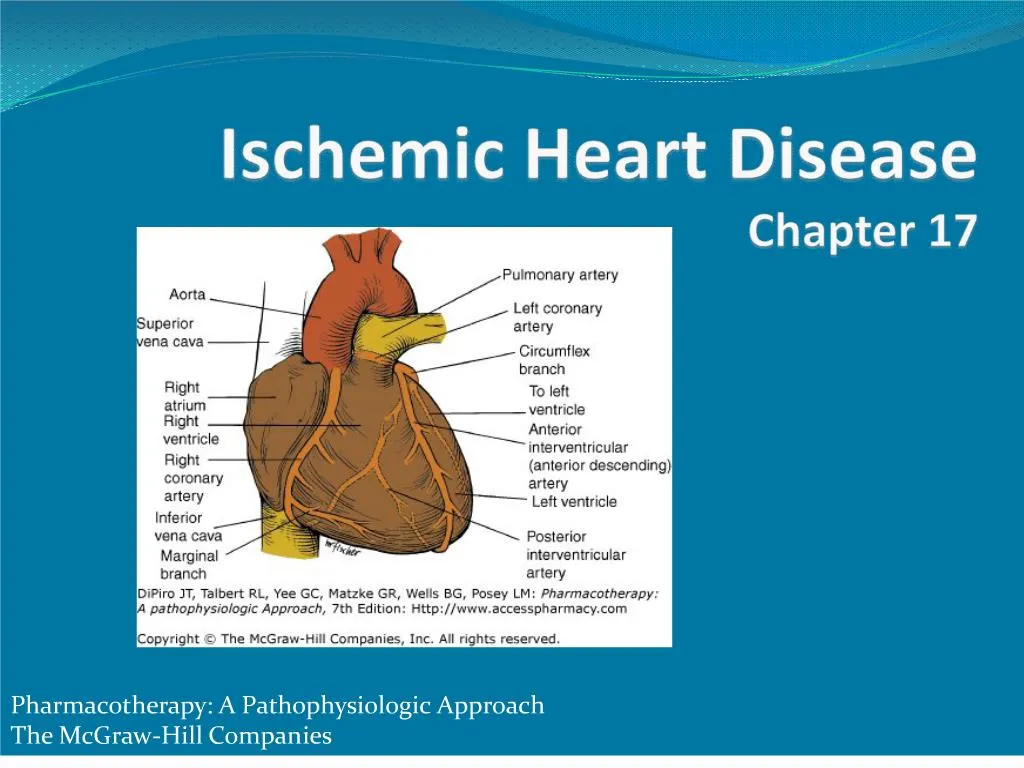
1. Ischemic Heart DiseaseChapter 17
2. 2
3. DCA: directional coronary atherectomy
ECG: electrocardiogram
EDRF: endothelium-derived relaxing factor
ETT: exercise tolerance (stress) testing
GMP: guanosine monophosphate
HDL: high-density lipoprotein
HERS: Heart Estrogen/Progestin Replacement Study
IHD: ischemic heart disease
I Na: late sodium current
ISDN: isosorbide dinitrate
ISMN: isosorbide mononitrate
3 Abbreviations
4. Abbreviations LAD: left anterior descending
LDL: low-density lipoprotein
LV: left ventricle
MI: myocardial infarction
MVO2: myocardial oxygen demand
PCI: primary coronary intervention
PTCA: percutaneous transluminal angioplasty
R1: resistance 1-large epicardial or surface vessels
R2: resistance 2-intramyocardial arteries and arterioles
4
5. Key Concepts Ischemic heart disease (IHD): caused by coronary atherosclerotic plaque formation which leads to imbalance between O2 supply & demand
results in myocardial ischemia
Chest pain: cardinal symptom of myocardial ischemia caused by coronary artery disease (CAD)
Risk factor identification/modification important interventions for patients with known/suspected IHD
5
6. Major risk factors that can be altered
dyslipidemia
high total & low-density lipoprotein cholesterol
low high-density lipoprotein cholesterol
high triglycerides
smoking
glycemic control in DM
HTN
therapeutic lifestyle changes
exercise, weight reduction, reduced dietary cholesterol
reduction in inflammation may play an important role
6 Key Concepts
7. Key Concepts Most CAD patients should receive antiplatelet therapy
Manage chronic stable angina patients initially with �-blockers for symptomatic control
at least as well as nitrates or CCBs
decrease risk of recurrent MI, CAD mortality
Nitroglycerin, other nitrate products useful for angina prophylaxis when patients undertake activities known to provoke angina
When angina occurs on a regular, routine basis
institute chronic prophylactic therapy
7
8. CCBs: effective monotherapy
generally used with �-blockers or as monotherapy for patients intolerant to �-blockers
most patients with moderate to severe angina require 2 drugs to control symptoms
ranolazine: 2nd line drug
used with �-blockers & CCBs 8 Key Concepts
9. Key Concepts Pharmacologic management as effective as revascularization if 1 or 2 vessels involved
no differences in survival
recurrent MI
other measures of effectiveness
Multivessel involvement best managed with revascularization
left main coronary artery disease
left main equivalent disease
2- to 4-vessel involvement with significant left ventricular dysfunction
9
10. Key Concepts Revascularization
percutaneous transluminal coronary angioplasty
coronary artery bypass graft (CABG)
certain patients (e.g. diabetics) should have CABG
Percutaneous transluminal coronary angioplasty & CABG produce similar results
10
11. BP
lipid profile
drug therapy hyperlipidemia
symptom & activity assessment
smoking cessation
antiplatelet therapy
�-blocker therapy for prior myocardial infarction
ACE inhibitor therapy
diabetes screening
11 Key Concepts
12. Ischemic Heart Disease Caused by epicardial vessel atherosclerosis which leads to coronary heart disease
Presentation:
acute coronary syndrome
chronic stable exertional angina pectoris
ischemia without clinical symptoms
heart failure, arrhythmias
cerebrovascular disease
peripheral vascular disease 12
13. Epidemiology ~79 million American adults: > 1 type of cardiovascular disease (CVD)
~2,400 Americans die of CVD each day
average of 1 death every 33 seconds
In 2004, CHD was responsible for 52% of CVD deaths
Common initial presentation:
women: angina
men: myocardial infarction
13
14. Criteria for Determination of the Specific Activity Scale Functional Class 14
15. 15
16. Angina Classified by symptom severity, disability, specific activity scale
Number of vessels obstructed important determinate of outcome
Risk factors for increased mortality:
heart failure
smoking
left main or left main equivalent CAD
diabetes
prior MI 16
17. Grading of Angina Pectoris by the Canadian Cardiovascular Society Classification System 17
18. Etiology/Pathophysiology Coronary atherosclerotic plaque formation leads to imbalance between O2 supply & demand ? myocardial ischemia
Ischemia: lack of O2, decreased or no blood flow in myocardium
Anoxia: absence of O2 to myocardium
18
19. Etiology/Pathophysiology Determinants of myocardial oxygen demand (MVO2)
HR
contractility
intramyocardial wall tension during systole (most important)
Determinants of ischemia:
resistance in vessels delivering blood to myocardium
MVO2
19
20. Etiology/Pathophysiology Coronary blood flow
inversely related to arteriolar resistance
directly related to coronary driving pressure
Extent of functional obstruction important limitation of coronary blood flow
severe stenosis (> 70%)
ischemia & symptoms at rest
21. 21
22. Etiology/Pathophysiology Changes in O2 balance lead to rapid changes in coronary blood flow
Mediators that affect O2 balance:
adenosine
other nucleotides
nitric oxide
prostaglandins
CO2
H+
23. Etiology/Pathophysiology Extrinsic factors
alterations in intramyocardial wall tension throughout the cardiac cycle
phasic systolic vascular bed compression
factors that favor reduction in blood flow
Intrinsic factors
myogenic control
Bayliss effect
neural components
parasympathetic nervous system, sympathetic nervoussystem, coronary reflexes
24. Etiology/Pathophysiology Factors limiting coronary perfusion:
coronary reserve diminished at ~85% obstruction
critical stenosis occurs when obstructing lesion encroaches on the luminal diameter & exceeds 70%
25. 25 Short-Term Risk of Death or Nonfatal Myocardial Infarction in Patients with Unstable Angina
26. Clinical Presentation of Angina Many ischemia episodes are silent (no symptoms)
Patients often have reproducible pattern, pain, other symptoms
Increased frequency, severity, duration, symptoms at rest suggests unstable angina
26
27. Clinical Presentation of Angina Symptoms
sensation of pressure/burning over or near sternum; often but not always radiating
left jaw, shoulder, arm
chest tightness, shortness of breath
visceral pain: lasts 0.5 to 30 min
precipitating factors: exercise, cold environment, walking after a meal, emotional upset, fright, anger, coitus
relief with rest, nitroglycerin
27
28. Clinical Presentation of Angina Signs
abnormal precordial systolic bulge
abnormal heart sounds
Typically no abnormal laboratory tests
Likely to have abnormal tests for IHD risk factors
History of chest pain
28
29. Differential Diagnosis of Episodic Chest Pain Resembling Angina Pectoris 29
30. 30
31. 31 Cardiac Findings in CAD Patients
32. 32
33. Diagnostic Tests Electrocardiogram (ECG)
normal in � of patients with angina not experiencing an acute attack
ST-T wave changes
depression
T-wave inversion
ST-segment elevation
significant ischemia
ST-segment depression > 2 mm
exertional hypotension
reduced exercise tolerance
33
34. 34
35. Diagnostic Tests Exercise Tolerance Testing (ETT)
recommended for patients with intermediate pretest probability of CAD based on age, gender, symptoms
insensitive for predicting coronary artery anatomy but correlates well with outcome
Echocardiography
useful if physical examination suggests valvular, pericardial disease, ventricular dysfunction
35
36. 36
37. Diagnostic Tests Cardiac imaging
radionucleotide angiocardiography
technetium pyrophosphate scans
positron emission tomography
ultrarapid computerized tomography
spiral CT
ultrafast CT
electron-beam CT
Cardiac catheterization & angiography
37
38. 38
39. 39
40. 40
41. IHD Treatment Short term goals:
reduce/prevent angina symptoms that limit exercise capability & impair quality of life (QOL)
Long-term goals:
prevent CHD events
MI
arrhythmias
heart failure
extend the patient�s life 41
42. 42
43. IHD Treatment Risk factor identification/modification
risk factors play a major role in determining occurrence & severity of IHD
risk factors are additive
classified as alterable or unalterable
43
44. IHD Treatment Unalterable risk factors:
gender
age
family history
environmental influences
climate, air pollution, trace metals in drinking water
diabetes mellitus
44
45. Alterable risk factors:
smoking
HTN
hyperlipidemia
obesity, sedentary lifestyle
hyperuricemia
psychosocial factors (stress, type A behavior)
medications
progestins
corticosteroids
cyclosporine
45 IHD Treatment
46. The American College of Cardiology and American Heart Association Evidence Grading System 46
47. Stable Exertional Angina Pectoris ASA (Class I, Level A)
�-blockers with prior MI (Class I, Level A)
ACE inhibitors for patients with CAD & diabetes or LV systolic dysfunction (Class I, Level A)
LDL-lowering therapy with CAD & LDL > 130 mg/dL (Class I, Level A)
target LDL < 100 mg/dL
< 70 mg/dL in patients with CHD & multiple risk factors
Sublingual nitroglycerin for immediate angina relief (Class I, Level B)
47
48. Stable Exertional Angina Pectoris Calcium antagonists or long-acting nitrates for symptom reduction when �-blockers contraindicated (Class I, Level B)
Calcium antagonists or long-acting nitrates in combination with �-blockers when initial �-blocker treatment is inadequate (Class I, Level C)
Calcium antagonists or long-acting nitrates as substitutes for �-blockers if initial �-blocker treatment leads to intolerable side effects (Class I, Level A)
48
49. Stable Exertional Angina Pectoris May substitute clopidogrel when ASA contraindicated (Class IIa, Level B)
Use of long-acting nondihydropyridine calcium antagonists instead of �-blockers as initial therapy (Class IIa, Level B)
Therapies to avoid:
dipyridamole (Class III, Level B)
chelation therapy (Class III, Level B)
49
50. Effect of Drug Therapy on Myocardial O2 Demand 50
51. Stable Exertional Angina Pectoris �-blocker place in therapy:
effective in chronic exertional angina as monotherapy and in combo with nitrates and/or CCBs
1st line in chronic angina that requires daily maintenance therapy
ideal candidates:
physical activity figures prominently in anginal attacks
coexistent hypertension
history of supraventricular arrhythmias or post-MI angina
anxiety associated with angina
51
52. Stable Exertional Angina Pectoris �-blockers
symptom control
reduce risk of recurrent MI, CAD mortality
may be used for chronic prophylaxis in patients with > 1 angina episodes/day
smokers have reduced anti-anginal efficacy
some have reduced efficacy based on lipid solubility
propranolol: lipid soluble, inducible metabolism
52
53. Stable Exertional Angina Pectoris �-blockers
overall effect of �-blockers in patients with effort-induced angina ? reduction in O2 demand
do not improve O2 supply
can blunt reflex tachycardia from nitrate therapy
may decrease exercise capacity in healthy individuals or those with HTN
may improve exercise tolerance in angina patients
53
54. Stable Exertional Angina Pectoris �-blockers
dosing based on t�
disparity between t� & duration of action for several BBs
renal/hepatic dysfunction affect disposition
route of elimination not major consideration in drug selection
54
55. Stable Exertional Angina Pectoris �-blocker adverse effects
abrupt withdrawal associated with increased severity & number of pain episodes & myocardial infarction
pharmacologic effects
CNS effects
fatigue
malaise
depression
55
56. chewable
oral
transdermal
ointments
spray
IV
56 Stable Exertional Angina Pectoris
57. Stable Exertional Angina Pectoris Nitrate therapy for acute attacks
sublingual
buccal
spray products
Symptom prophylaxis when undertaking activities that precipitate attacks
oral or transdermal products
0.3 to 0.4 mg SL ~5 min prior to activity
Chronic prophylaxis with long-acting forms
tolerance: limiting factor
57
58. Stable Exertional Angina Pectoris Nitrate therapy
reduces MVO2 2? to venodilation & arterial-arteriolar dilation ? reduction in wall stress from reduced ventricular volume & pressure
systemic venodilation increases flow to deep myocardial tissue
dilation of large & small intramural coronary arteries, collateral dilation, coronary artery stenosis dilation, abolition of normal tone in narrowed vessels, relief of spasms
58
59. Stable Exertional Angina Pectoris Nitrate therapy
large 1st-pass effect
short t� (except isosorbide mononitrate)
see Nitrate Products chart on slide 61
large volume of distribution
high clearance rates
large interindividual variation in plasma/blood concentrations
saturable metabolism
accumulation of metabolites with multiple doses
drug adsorption to PVC tubing, syringes
59
60. Stable Exertional Angina Pectoris Nitrate therapy adverse effects
extension of pharmacologic effects
postural hypotension with CNS symptoms, headaches, flushing 2? to vasodilation
occasional nausea from smooth muscle relaxation
reflex tachycardia, but bradycardia has been reported
rash with all products (particularly with patches)
production of methemoglobinemia with high doses for extended periods
measurable ethanol & propylene glycol concentrations with IV nitroglycerin
tolerance
60
61. Nitrate Products 61
62. Stable Exertional Angina Pectoris Calcium channel blockers (CCBs)
effective monotherapy (usually used if patients are intolerant of �-blockers)
generally used in combination with �-blockers
improve coronary blood flow through coronary artery vasodilation, decrease MVO2
provide better skeletal muscle oxygenation than �-blockers ? decrease fatigue, improve exercise tolerance
CCBs have similar efficacy
differences in electrophysiology, peripheral/central hemodynamic effects, ADR profiles useful in selecting appropriate agent
62
63. Stable Exertional Angina Pectoris Calcium channel blockers (CCBs)
ideal candidates
contraindications/intolerance to �-blockers
coeixting conduction system disease (except verapamil, diltiazem)
Prinzmetal angina
peripheral vascular disease
severe ventricular dysfunction (amlodipine drug of choice)
concurrent HTN
63
64. Stable Exertional Angina Pectoris Calcium channel blockers (CCBs)
vasodilation of systemic arterioles & coronary arteries
reduction of arterial pressure and coronary vascular resistance
depression of myocardial contractility & conduction velocity of the SA/AV nodes
MVO2 reduction due to reduced wall tension 2? to reduced arterial pressure
may improve coronary blood flow through areas of fixed coronary obstruction
inhibits coronary artery vasomotion/vasospasm
non-dihydropyridine products affect AV conduction and contractility
64
65. Stable Exertional Angina Pectoris Calcium channel blockers (CCBs)
large, variable, 1st-pass metabolism
~20 to 50% bioavailability for diltiazem, nicardipine, nifedipine, verapamil, felodipine, isradipine
amlodipine bioavailability ~60 to 80%
most CCBs eliminated via CYP 3A4 & other CYP isoenzymes
65
66. Stable Exertional Angina Pectoris Ranolazine
reduces Ca2+ overload in ischemic myocytes through selective inhibition of late Na+ current (INa)
does not affect HR, inotropic state, hemodynamic state or increase coronary blood flow
indicated for chronic angina treatment
prolongs QT interval
reserved for patients who have not achieved adequate response with other antianginal agents 66
67. Ranolazine
dose: 500 mg BID then 1000 mg BID
contraindications
preexisting QT interval prolongation
hepatic impairment
drug interactions
other QT interval-prolonging medications
cytochrome P450 3A inhibitors decrease ranolazine clearance
67 Stable Exertional Angina Pectoris
68. Clinical Controversy MERLIN-TIMI 36
Metabolic Efficiency With Ranolazine for Less Ischemia in Non-ST-Elevation Acute Coronary Syndromes
Randomized, double-blind, controlled trial (n=6560)
2 groups
ranolazine 1000 mg BID
placebo
68
69. MERLIN-TIMI 36 results
NSTEMI angina symptom relief
6.2% HbA1c reduction at 4 months: ranolazine group
5.9% HbA1c reduction at 4 months: placebo
0.30 versus 0.04 (p<0.001) � clinical significance?
no significant reduction in composite 1� outcome at (median follow-up 348 days)
CV death
MI, recurrent ischemia
69 Clinical Controversy
70. 70
71. 71
72. Stable Exertional Angina Pectoris Nonpharmacologic therapy
revascularization
coronary artery bypass grafting
percutaneous transluminal coronary angioplasty
72
73. 73 Recommended Mode of Coronary Revascularization��
74. 74
75. Stable Exertional Angina Pectoris Revascularization
based on extent of coronary disease (# of vessels, location/amount of stenosis) & ventricular function
complications: coronary artery spasm, intraluminal thrombus
combination therapy with acetylsalicylic acid, unfractionated heparin, or low-molecular-weight heparin, glycoprotein IIb/IIIa receptor antagonists & stents have reduced occurrence of reocclusion & late restenosis
75
76. Stable Exertional Angina Pectoris Coronary artery bypass grafting (CABG)
reduces symptomatic angina not controlled by medical management or PCI
improves patient lifestyle
reduces CAD mortality
reduces need for nitrates, �-blockers
76
77. Stable Exertional Angina Pectoris Percutaneous transluminal coronary angioplasty (PTCA)
reduced stenosis due to
compression, redistribution of plaque
embolization of plaque contents
aneurysm formation
disruption of plaque & arterial wall
patients usually heparinized during PTCA to prevent immediate thrombus formation at site of arterial injury
anticoagulation up to 24 hrs
77
78. Stable Exertional Angina Pectoris Percutaneous transluminal coronary angioplasty (PTCA)
prevention of restenosis:
combination therapy with acetylsalicylic acid, heparin, GP IIa/IIIa receptor antagonists
bivalirudin
drug-eluting & bare metal stents
78
79. Stable Exertional Angina Pectoris PTCA vs CABG
low-risk patients have greater alleviation of symptoms with PTCA
moderate-risk patients had equal mortality & MI rates with PTCA or CABG
high-risk patients showed improved survival with CABG than medical therapy
79
80. Stable Exertional Angina Pectoris Drug-eluting stents
sirolimus (Cypher�)
paclitaxel (Taxus�)
zotarolimus (Endeavor�)
target revascularization needed less often than bare stents
combination antiplatelet therapy (ASA + clopidogrel) for > 1 yr following implantation
80
81. Drug-eluting stents Antiplatelet therapy often discontinued in surgical patients with drug-eluting stents
risk factor for late stent thrombosis
Medline search for late & very late stent thrombosis cases Jan 2001 to July 2008
When patients stopped antiplatelet agents simultaneously, median time to event: 7 days
If the thienopyridine was stopped & ASA continued, median time to event: 122 days
81
82. Variant Angina Pectoris Prinzmetal angina
associated with ST-segment elevation
commonly resolves without progression to MI
usually younger patients
82
83. Variant Angina Pectoris Causes
imbalance between endothelium-produced vasodilator factors (prostacyclin, nitric oxide) & vasoconstrictor factors (endothelin, angiotensin II)
imbalance of autonomic control characterized by parasympathetic dominance of inflammation
adrenoreceptor polymorphisms may predispose patients to developing vasospasm 83
84. Variant Angina Pectoris Precipitating factors
hyperventilation
exercise
exposure to cold
May have no apparent precipitating cause
84
85. Coronary Artery Spasm Diagnosis
ST-segment elevation during transient chest discomfort (usually at rest) that resolves when chest discomfort diminishes in patients with normal or non-obstructive lesions
In absence of ST-segment elevation, may use provocative tests to precipitate coronary artery spasm
ergonovine, acetylcholine, methacholine
withdraw nitrates & CCB prior to testing
85
86. Coronary Artery Spasm Treatment
optimization of therapy includes dose titration
treat all patients for acute attacks
maintain prophylactic treatment 6 to 12 months following initial episode
eliminate aggravating factors
alcohol
cocaine
cigarette smoking
86
87. Coronary Artery Spasm Treatment
nitrates for acute attacks
CCBs
nifedipine, verapamil, diltiazem equally effective single agents for initial treatment
dose titration needed
combination therapy with nifedipine-diltiazem or nifedipine-verapamil useful for patients unresponsive to single-drug regimens
�-blockers have little or no role
87
88. Silent Ischemia Associated with ST-segment elevation, depression
Frequently occurs without antecedent HR, BP changes
ischemia from reduction in O2 supply
2 classes
Class I: patients do not experience angina
Class II: patients have both asymptomatic & symptomatic ischemia
Associated with reduced survival, increased need for PTCA/CABG, increased risk of acute MI
88
89. Silent Ischemia Causes
increased physical activity
sympathetic nervous system activation
? cortisol secretion
? coronary artery tone
enhanced platelet aggregation due to endothelial dysfunction leading to intermittent coronary obstruction 89
90. Silent Ischemia Diagnosis: ambulatory ECG
Initial management
modify IHD risk factors
HTN
hypercholesterolemia
smoking
Treatment goal
reduce number of ischemic episodes (symptomatic & asymptomatic), regardless of direction of ST-segment shift
90
91. Silent Ischemia Pharmacologic treatment
�-blockers
most useful for post-MI patients or those with high level of sympathetic nervous system activity
CCBs alone or in combination effective in reducing symptomatic & asymptomatic ischemia
do not interrupt diurnal surge in ischemia
less effective than �-blockers
combination �-blockers & CCBs: better response than CCBs & nitrates or CCB monotherapy 91
92. Therapeutic Outcomes Angina symptom improvement
Improved cardiac performance
Risk factor reduction
Increased exercise capacity
May use coronary angiography to assess extent of stenosis or restenosis after angioplasty or CABG 92
93. Clinical Controversy Many long-term trials compare �-blockade vs CCBs to determine superior survival benefit
�-blockers recommended 1st line prophylactic therapy for symptomatic angina patients requiring daily pharmacologic therapy
effective in post-MI patients
favorable adverse effect profile
Stable CAD: medical management produces outcomes similar to revascularization
may impact future use of healthcare resources
93
94. Recent developments in understanding organic nitrates bioactivation raise concern over endothelial dysfunction induced by long-term nitrate administration
Nitrate products activated via different mechanisms
impacts long-term effectiveness of individual drugs
94 Clinical Controversy
95. 95 American College of Cardiology, American Heart Association, and Physician Consortium for Performance Improvement Chronic Stable Coronary Artery Disease Core Physician Performance Measurement Seta
96. 96 American College of Cardiology, American Heart Association, and Physician Consortium for Performance Improvement Chronic Stable Coronary Artery Disease Core Physician Performance Measurement Seta
97. 97 American College of Cardiology, American Heart Association, and Physician Consortium for Performance Improvement Chronic Stable Coronary Artery Disease Core Physician Performance Measurement Seta
98. Table Footnotes aRefers to all patients diagnosed with CAD
bMedical reasons for not prescribing antiplatelet therapy (aspirin, clopidogrel, or combination of aspirin and dipyridamole): active bleeding in the previous 6 months with required hospitalization and/or transfusion(s), patient on other antiplately therapy, etc.
Medical reasons for not prescribing a statin: clinical judgement, documented LCL-C < 130 mg/dL, etc.
Medical reasons for not prescribing a �-blocker: bradycardia (defined as heart rate < 50 beats/min without �-blocker therapy), history of class IV (congestive) heart failure, history of second- or third-degree atrioventricular block without permanent pacemaker, etc.
Medical reasons for not prescribing ACE inhibitor (ACEI): allergy, angioedema caused by ACEI, anuric rental failure caused by ACEI, pregnancy, moderate or severe aortic stenosis, etc.
cPatient reasons for not prescribing antiplatelet therapy, statin, -blocker, or ACEI: economic, social, and/or religious, etc.
dAntiplatelet therapy may include aspirin, clopidogrel, or combination of aspirin and dipyridamole.
eNot indicated for a statin refers to LCL-C < 100 mg/dL.
fTest measure.
gScreening for diabetes is usually done by fasting blood glucose or 2-hour glucose tolerance testing. Clinical recommendations indicate screening should be considered at 3-year intervals.
98
99. Acknowledgements
Prepared By: Amy Pai, Pharm.D.
Series Editor: April Casselman, Pharm.D.
Editor-in-Chief: Robert L. Talbert, Pharm.D., FCCP, BCPS, FAHA
Chapter Author/Section Editor:
Robert L. Talbert, Pharm.D., FCCP, BCPS, FAHA 99






















