Download
1 / 39
420 likes | 740 Views
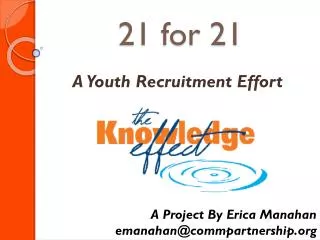
Case 21. 32 year old white male had elective colonoscopy based on a family history of colon cancer Colonoscopy: superficial hemorrhagic lesions in the sigmoid, descending, and transverse colon, and terminal ileum. Staging for lymphoma was negative including bone marrow exam

E N D
Case 21 • 32 year old white male had elective colonoscopy based on a family history of colon cancer • Colonoscopy: superficial hemorrhagic lesions in the sigmoid, descending, and transverse colon, and terminal ileum. • Staging for lymphoma was negative including bone marrow exam • Clinical evaluation for celiac disease showed high titers of antigliadin IgA and IgG antibodies, but negativity for tissue-transglutaminase • Minor response to gluten free diet
Appearance of lesion on endoscopy Colon Biopsy 2002
CD3 CD56
CD2 TIA-1
Case 21 – Follow Up • Over 8 years: similar lesions in the large bowel, stomach and small intestine. • Some lesions have waxed and waned, but there has been no progression of disease • A minor population of similar appearing cells was identified in tonsil • Peripheral blood flow has been normal
CD56 Index case reported as: Indolent NK-cell Lymphocytosis of the GI tract (Vega et al. AJSP 2006)
Proposal for a A New Clinical Entity - NK-cell EnteropathyMansoor, A., S. et al. Blood 2011 • 8 cases: M:F 1:3; Median age 49 (27-70) • Vague GI symptoms, but negative for celiac disease • Single site of involvement in 3 patients • Stomach, colon(2) • Multiple sites in 5 patients • Stomach, small intestine, colon • Superficial lesions with hemorrhage, edema, ulceration
CD56 Case 4: Duodenal biopsy in 53 y.o. Male, with gastric and duodenal lesions, persistent at 2 yrs.
Immunophenotype: NK-cell Enteropathy • EBV-negative • CD56 strongly + • TIA-1+/ GrB+ • cCD3+, CD7 + • T-cell ag negative: CD4, CD8, CD5, βF1 CD2 variable • PCR neg for TCR gene rearrangement PB and BM: normal in all six studied
NK-cell Enteropathy - Follow Up • 6/7 patients with repeat endoscopy had persistent but non-progressive disease • Follow up (median 34 mos; 8 yrs in index case, longest 10 years) • 3 pts had CHOP chemotherapy, in 2 pts followed by auto BMT • 2 have persistent GI lesions following treatment • 1 pt is currently NED at 1yr • No evidence of BM involvement or spread outside the GI tract
Similar reports in literature • Takeuchi et al. Blood 2010 • Lymphomatoid gastropathy • 10 cases, adults, M=F, often for evaluation for gastric cancer, no intestinal involvement seen • McElroy et al. Ann Diag Pathol 2010 • 52 yo female, lesions in colon and stomach • Negative evaluation for celiac disease • Persistent GI involvement but without progression • Yamamoto et al, In press • 70 yo male, gastric ulcers, self limited course
Differential Diagnosis • Extranodal NK/T-cell lymphoma • EBV +, NK-cell phenotype, CD56+, CD3c • Clinically aggressive • EATL, type II (monomorphic) • CD56+, but γδ T-cell phenotype, clonal PCR • Worldwide distribution, not linked to celiac disease • EATL, type I • Associated with celiac disease, clonal PCR • Cytotoxic αβ T-cell phenotype • Gamma-delta TCL • CD56+, γδ T-cell phenotype, clonal PCR • Some but not all cases resemble EATL type II
Extranodal NK/T Cell Lymphoma, Nasal-typeClinical Presentation • “Lethal Midline Granuloma” • most common clinical presentation • Nasal septum, palate • Midline facial structures, orbit • Skin and subcutaneous sites • GI tract • Testis • Lung (uncommon)
Enteropathy Associated T-cell Lymphoma I (EATL I) • Broad morphological spectrum • Adjacent mucosa shows villous atrophy • CD3+, CD103+, Cytotoxic markers, TCR ab • often double negative for CD4/CD8, CD56 usu - • Often presents with intestinal perforation • aggressive clinical course with poor prognosis
Enteropathy-associatedT-Cell Lymphoma • Associated with celiac disease • 95% of patients have HLA-DQ2 encoded by HLA DQA10501, DQB10201 • Gluten-free diet may reduce risk • In some patients, lymphoma may be the presenting feature
Monomorphic type (Type II) • Medium sized cells with clear cytoplasm • CD56 +, CD8+, CD4- • 8q24 (myc) amplifications • May occur sporadically, without celiac disease • Likely an independent entity (In WHO 2008 still included as subtype of EATL)
EATL in Hong KongChan et al. AJSP 2011 • 18 cases – all EATL Type II (monomorphic) • 13 males/ 5 females Median age: 62 • No history of malabsorption • All EBV negative • 14 (78%) gamma delta • 6 (33%) alpha beta • 3 cases dual positive, 1 case TCR silent
γδ T-cell Lymphomas- Comparison of Clinical & Pathological Features (WHO 2008) Hepatosplenic gdPrimary Cutaneous gd Children, Young adults, M>>F Adults, M=F Liver, spleen Skin, Subcutaneous tissue Bone marrow ? Other extranodal sites Aggressive Aggressive Immature cytotoxic Mature or activated cytotoxic phenotype phenotype TIA-1 +, Granzyme B - TIA-1+, Granzyme B +, Perforin + Perforin neg
Non-hepatosplenic gamma/delta T-cell Lymphomas Garcia-Herrera et al. AJSP 2011 • 27 PTCL suspected of being gd TCL were studied in paraffin with abs to TCR d or TCR g • Cases contributed from Barcelona, Spain; NCI, Bethesda; Taipei, Taiwan; Creteil, France • All confirmed to have TCR genes clonally rearranged • EBV positive in 3/27 • 2 skin, 1 nodal
Non-hepatosplenicgd T-cell lymphomas (16)Sites of Presentation • Skin / subcutaneous tissue (5) 31% • Skin + other (GI, LN) (3) 19% • Small bowel (3) 19% • Tongue (1) 6% • Orbit (1) 6% • Lung (1) 6% • LN (2) 12% 50%
γδ TCL 26 yo Hispanic male
CD3 CD5
PTCL, TCR silent (11 cases) • TCR gamma rearranged by PCR • Negative for Beta F1, TCR delta & TCR gamma • Clinically similar to gd TCL • 6/11 skin & subcutaneous tissue • 3/11 small bowel • 1 each, LN and CNS TCR Silent and gdTCL: 75% DOD, median < 2 yr
Intestinal T-cell Lymphomas 6/6 males; Median age 58 (49-72) 5/6 Asian; 1 Hispanic All cytotoxic: CD56+, CD3+, CD8+, CD7+ All CD5 negative, EBV negative 3 gamma delta; 3 were TCR silent 2/6 had morphological features of EATL, Type II 1 Asian, 1 Hispanic 4/6 lacked prominent epitheliotropism
Intestinal T-cell/ NK-cell LymphomasA heterogeneous spectrum of disease • Aggressive lymphomas with a cytotoxic T-cell or NK-cell phenotype • Enteropathy associated T-cell lymphoma (type I) • EATL, Type II (monomorphic type) • Predominantly gd origin • Not linked to celiac disease • Other cytotoxic TCL (gd and TCR silent) • Nasal type T/NK-cell lymphoma, EBV+
NK-cell enteropathy is a indolent disease of unknown etiology • This could represent an immune response to an unknown pathogen • The cytological atypia and CD56+ often leads to a mistaken dx of NK-cell or T-cell lymphoma • Be cautious about making the diagnosis of lymphoma on superficial biopsies


![[Case Study] 21 Growth Hacking Stories](https://cdn4.slideserve.com/8163028/case-study-21-growth-hacking-stories-dt.jpg)