Download
1 / 30
300 likes | 635 Views
Modeling the Ebola Outbreak in West Africa, 2014. Sept 30 th Update Bryan Lewis PhD, MPH ( blewis@vbi.vt.edu ) Caitlin Rivers MPH, Eric Lofgren PhD, James Schlitt , Katie Dunphy , Henning Mortveit PhD, Dawen Xie MS, Samarth Swarup PhD, Hannah Chungbaek ,

E N D
Modeling the Ebola Outbreak in West Africa, 2014 Sept 30th Update Bryan Lewis PhD, MPH (blewis@vbi.vt.edu) Caitlin Rivers MPH, Eric Lofgren PhD, James Schlitt, Katie Dunphy, Henning Mortveit PhD, DawenXie MS, Samarth Swarup PhD, Hannah Chungbaek, Keith Bisset PhD, Maleq Khan PhD, Chris Kuhlman PhD, Stephen Eubank PhD, MadhavMarathe PhD, and Chris Barrett PhD
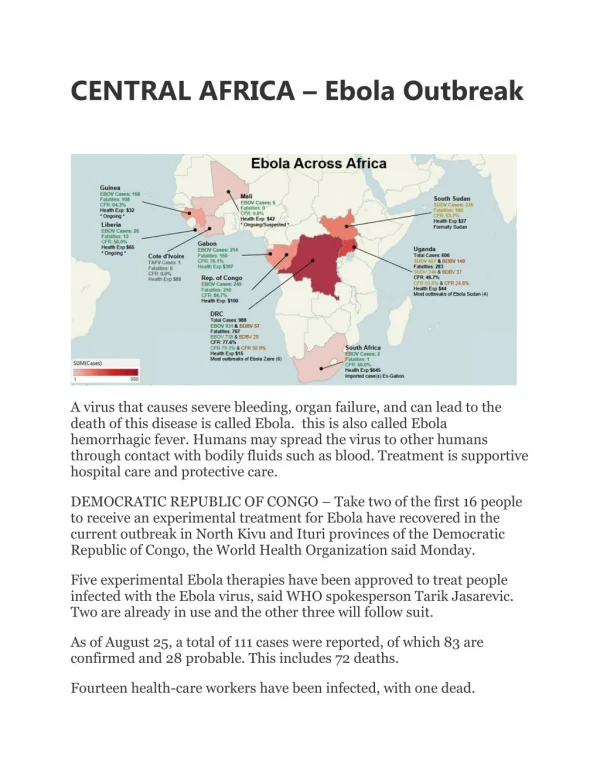
Currently Used Data Cases Deaths Guinea 1074648 Liberia 33621830 Nigeria 22 8 Sierra Leone 2208605 Total 66663091 • Data from WHO, MoH Liberia, and MoH Sierra Leone, available at https://github.com/cmrivers/ebola • MoH and WHO have reasonable agreement • Sierra Leone case counts censored up to 4/30/14. • Time series was filled in with missing dates, and case counts were interpolated.
Epi Notes • Reports of efficacy of HIV drug “” lowering mortality CNN • Two other physicians infected with Ebola back in US, one at NIH enrolled in vax trial Politico • Suspect cases continue to be identified in the US, currently a patient in Dallas (previous negatives from CA, NY, NM, FL) WaPo • Sierra Leone’s reporting still inconsistent Crawford Killian
Liberia Forecasts Forecast performance 52% of Infected are hospitalized Reproductive Number Community 1.3 Hospital 0.4 Funeral0.5 Overall 2.2
Sierra Leone Forecasts Forecast performance 41% of cases are hospitalized
All Countries Forecasts rI: 1.1 rH:0.4 rF:0.3 Overall:1.7
Experiments • Hospital bed estimate calculations • Reduction in time to hospitalization • Improvements in time from symptom onset to hospitalization
Hospital Beds – Prelim analysis Impact in Liberia, beds only Cases on Feb 1 Oct 1 245k Nov 1 312k Dec 1 391k Jan 1 475k No beds 533k 16% hospitalization ratio -> 70% Beta_H reduction by 90%
Hospital Beds – Prelim analysis Impact in Liberia, beds and proper burial Cases on Feb 1 Oct 1 73k Nov 1 135k Dec 1 230k Jan 1 375k No beds 533k 16% hospitalization ratio -> 70% Beta_H reduction by 90% Beta_F reduction by 90%
Hospital beds – Prelim analysis Impact in Liberia, beds + proper burial + shortened time to hospitalization
Hospital beds – Prelim analysis Cumulative cases in Liberia on Feb 1 with reduced beta_H, reduced beta_F, and shortened time to hospitalization
Optimal center placement Preliminary optimization using road networks and population centers
Agent-based Simulations Progress • Regional travel method, developed • Implementation working this week • Interventional support designed for • Increasing hospitalization level • Better burial • Decreasing time to hospitalization • Capacity monitoring at ETU/ECU designed • Need some bounds on experimental design
Supporting material describing model structure, and additional results Appendix
Legrand et al. Model Description Legrand, J, R F Grais, P Y Boelle, A J Valleron, and A Flahault. “Understanding the Dynamics of Ebola Epidemics” Epidemiology and Infection 135 (4). 2007. Cambridge University Press: 610–21. doi:10.1017/S0950268806007217.
Compartmental Model • Extension of model proposed by Legrand et al. Legrand, J, R F Grais, P Y Boelle, A J Valleron, and A Flahault. “Understanding the Dynamics of Ebola Epidemics” Epidemiology and Infection 135 (4). 2007. Cambridge University Press: 610–21. doi:10.1017/S0950268806007217.
Legrand et al. Approach • Behavioral changes to reduce transmissibilities at specified days • Stochastic implementation fit to two historical outbreaks • Kikwit, DRC, 1995 • Gulu, Uganda, 2000 • Finds two different “types” of outbreaks • Community vs. Funeral driven outbreaks
NDSSL Extensions to Legrand Model • Multiple stages of behavioral change possible during this prolonged outbreak • Optimization of fit through automated method • Experiment: • Explore “degree” of fit using the two different outbreak types for each country in current outbreak
Optimized Fit Process • Parameters to explored selected • Diag_rate, beta_I, beta_H, beta_F, gamma_I, gamma_D, gamma_F, gamma_H • Initial values based on two historical outbreak • Optimization routine • Runs model with various permutations of parameters • Output compared to observed case count • Algorithm chooses combinations that minimize the difference between observed case counts and model outputs, selects “best” one
Fitted Model Caveats • Assumptions: • Behavioral changes effect each transmission route similarly • Mixing occurs differently for each of the three compartments but uniformly within • These models are likely “overfitted” • Many combos of parameters will fit the same curve • Guided by knowledge of the outbreak and additional data sources to keep parameters plausible • Structure of the model is supported
Long-term Operational Estimates • Based on forced bend through extreme reduction in transmission coefficients, no evidence to support bends at these points • Long term projections are unstable