Download
1 / 100
1k likes | 1.04k Views
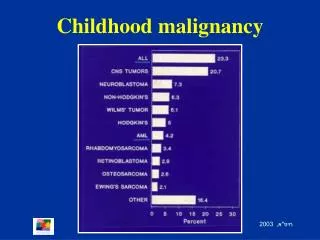
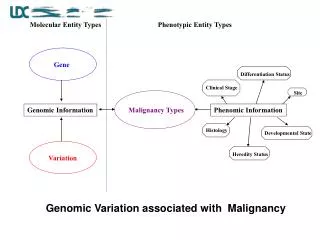
LABORATORY EXAMINATION OF ABDOMINAL MALIGNANCY. Dr. . dr. Siti Muchayat , MS, Sp PK (K). ONCOGENESIS. Growth promoting oncogenes. Tumor suppressor genes. Care taker genes. Activation Amplific Mutations. Inactivation Mutations. Transformation Uncontrolled growth, Abn biol behaviour

E N D
LABORATORY EXAMINATION OF ABDOMINAL MALIGNANCY Dr. . dr.Siti Muchayat , MS, Sp PK (K)
ONCOGENESIS Growth promoting oncogenes Tumor suppressor genes Care taker genes Activation Amplific Mutations Inactivation Mutations Transformation Uncontrolled growth, Abnbiolbehaviour Maturation arrest Abnormal diff
CELLULAR ALTERATIONS IN NEOPLASTIC CELLS Loss of contact inhibition Loss of adhesion Loss of cohesian Loss of normal Ag Surface changes - electrical charge - surface glycoprot Cytopl changes • loss of microtubules • synthesis of tumor products New tumor associated Ag - viral - oncofetal Karyotypic Changes: -oncogene -aneuploidy -marker chromosome Nuclei : • hyperchromatic • enlarged nucleus • enlarged nucleoli
Setiap sel mempunyai mekanisme pertahanan ► untuk tidak menjadi sel kanker ► dengan beberapa gene independent. Tumor dapat berkembang ► o.k. Mutasi yang berulang pada semua gene dalam sel. Lesi prakanker ► dapat sembuh menjadi tumor jinak menjadi tumor ganas
TUMOR DEVELOPMENT AND METHODS OF DETECTION Diagnostic threshold “early” “late” Long “invisible” preliminary stage months to many years 1 kg 1012 cells 10 - 100 g 1010 - 1011 cells 1 g 109 cells 1 mg 106 cells 1 mcg 103 cells Immunological methods Biophysical methods
BIOKIMIA SEL TUMOR Perubahan dalam inti sel Perubahan struktur kromosom Perubahan protein yang berkaitan dengan DNA Modifikasi t-RNA Pola enzim terdiferensiasi Perubahan dalam sitoplasma Terbentuk (sintesa) protein oncofetal masuk sirkulasi Perubahan pada permukaan sel Terbentuk Ag baru Hilang nya Ag lama Perubahan struktur glikoprotein (shg mengubah transpor ke dalam sel & permeabilitas sel) Communication between cells is reduced (thus changing the power of adhesion andinhibit contact between cells)
PENANDA TUMOR Senyawa spesifik (dalam sirkulasi) yang dihasilkan sel-sel ganas atau produk sekunder akibat pertumbuhan sel ganas. Penanda tumor yang Ideal Berkaitan dg proses keganasan Mempunyai korelasi dg masa tumor Dapat menunjukkan tipe, lokasi, dan stadium tumor Bisa menggambarkan efek terapi Mampu meramalkan prognosis penyakit Dapat meramalkan terjadinya kekambuhan/ metastasis Sampai saat ini belum ada PT ideal o.k. Heterogenitas dan komplexitas pertumbuhan sel ganas.
Pananda Tumor Dibedakan: • Produk yang dihasilkan oleh sel tumor itu sendiri Contoh: - Carcinoembryonic Antigen (CEA) - Alfa fetoprotein (AFP) Senyawa jg dihasilkan sel normal tp dgn jlh yg kecil 2. Produk yang menyertai proses keganasan Senyawa yg dibtk sekunder sbg akibat proses keganasan Contoh: - Carbohydrate Antigen 19-9 (CA 19-9) - Cancer Antigen 125 (CA 125)
Penanda tumor Produk Asal Tumor Produk Penyerta Tumor Hasil Sintesa Substansi aktif Parameter serum enzim jaringan metabolik berubah sehat masuk sirkulasi Onkofetal Ag (AFP, CEA, TPA) Enzim (GGT, LDH, ALP, AP) CA 19-9 Ag Onkoplacental (HCG, SP1) Hormon (Gastrin, insulin) CA 125 Ag Ektopik (enzim; glikolisis Metabolit (feritin, β2-mikroglobulin) MCA Sintesa protein, sintesa as.nukleat) PAP
Sampai saat ini tes yang mampu untuk surveilance HCC adalah Serum αfetoprotein dan hepatic ultrasonografi. Kadar AFP mempunyai sensitivitas dan spesifisitas rendah . Ultrasonografi ; tergantung dan terbatas kemampuannya membedakan HCC dengan non neoplastik . Dikembangkan biomarker sebagai indikator proses biologi’: selular, biokimia, molekular, perubahan genetik Selama tahun 2000-2009 dikembangkan 2784 penelitian; gene dan protein expression microarray, proteomic, tumor imunologi,
PENDAHULUAN Hepatocellular carcinoma (HCC) keganasan banyak terdapat di dunia. Insiden : range <10 kasus per 100,000 populasi di North America danWestern Europe seperti di Iran, Iraq dan India 50 – 150 kasus per 100,000 populasi di bagian Africa dan Asia. HCC : Sebagian besar mengakibatkan kematian. Dengan meningkatnya insiden dan mortalitas HCC, merefleksikan peningkatan prevalensi hepatitis C virus (HCV) infeksi.
Major etiologies of HCC. Chronic hepatitis B, C, and D Toxins (e.g., alcohol, tobacco, aflatoxins) Hereditary metabolic liver diseases (e.g., hereditary hemochromatosis, a1 antitrypsin deficiency) Autoimmune hepatitis State of insulin resistance Overweight in males Diabetes mellitus Nonalcoholicsteatohepatitis (NASH) or nonalcoholic Fatty liver disease (NAFLD)
Single Marker Α Fetoprotein * Fetal globulin disintesa sbgn besar di jaringan hati embryonal dan sel yolk sac di sekresi ke serum semasa janin. AFP hilang ses bayi berumur 6 minggu dan pd orang normal. Prinsip Pem: Cara immunodifusi kepekaan sampai 5 g/l. Cara counter imunoelektroforesis kepekaan sampai 100 mg/ml. Cara pasive haemagglutinasi 30 ng/ml. RIA 2-5 ng/ml.
AFP Positip pada; • primer hepatoma 40-80% (imunodifusi), 80-90% (RIA). - Juga pd teratoblastoma gonad, ataxia telengiectasis, hepatitis infeksiosa, Ca hati metastatik, Ca lambung. - Prognosa pd Tx surgikal, radiasi, chemoterapi dari hepatoma. - Pada sirosis meramal adanya hepatoma. - Meningkat pd regenerasi yang hebat dari sel-sel hati, mis; hepatektomi partial, hepatitis yang parah
AFP ☻ Sensitivitas antara 39%-65%, spesifisitas 76%-97% Variasi sangat tinggi o.k. Pada penelitian yang berbeda menggunakan cut-off yang berbeda dan juga penelitian yang retrospektif. ☻ Dapat diandalkan dengan menggunakan cut-off > 400 IU/ml, nilai ini sangat tinggi persentase sangat kecil kejadian HCC. ☻ Penting disini batasan dari marker ini.
AFP- L3 • Varian fucosylat ( tambahan a1-6 fucose residu) dari glikoprotein AFP yang mempunyai affinitas tinggi pada rantai glukosa dari lens culinaris. • Dipakai diagnosis HCC sebagai; Lens culinaris agglutinin-reactive α-fetoprotein. • AFP- L3 adalah AFP-L3% (rasio AFP-L3 : total AFP) secara lectin-affinity elektrophoresis, band diukur dg densitometer. • Mempunyai korelasi dengan staging HCC Berkorelasi dengan prognosis penderita HCC Berhubungan dengan menurunnya fungsi hati, differensiasi yang buruk, karakteristik biologi dari HCC. HCC yang kecil < 2 cm follow-up perjalanan penyakit & evaluasi terapi
Sensitivitas dan Spesifisitas Cut-off 10% sensi 36,1% spesi 93,4% 15% sensi 30,9% spesi 99,5% 15% sensi 55,3% spesi 93,9% 35% sensi 75% spesi 83% Penelitian terakhir : Cut-off 15% sensi 96% dan spesi 92% Inkonsistensi hasil karena sulit menstandarkan hasil konversi data kualitatif dari imunobloting dg densitometer
Carcino Embryonic Antigen CEA * Glycoprotein yang dihasilkan jaringan embryonal & jaringan neoplastik sistem GI. * Prinsip pem: Cara RIA * Harga normal < 2,5 ng/ml.
* Interpretasi - Mepd ; kronikaktiv hepatitis (22%), hepatoma (63%), sirosisalkoholik (88%). - Adakorelasi dg derajatgangguan fungsihati(ALP, GOT). - Tertinggi pd Ca colon, Ca pankreas (50%)4X nilai N. Utkprognosa post reseksi Ca colorectal. Metastasekehati CEA 4X nilai N.
ANTI p 53 Antibodi P53 adalah protein tumor suppressor yang diproduksi gene p53. Pada keganasan didapatkan konsentrasi tinggi p53 protein mutasi dengan paruh waktu terpanjang. Diawali dengan mutasi protein jangka waktu lama terbentuk auto antibodi yaitu anti-p53. Kelemahan anti p53: Tidak sensitif untuk HCC 20-25% 100% positif pada Cholangiocarcinoma, juga pada keganasan: gaster, pancreas, esofageal, dan colon.
Des-Gamma Carboxy Prothrombin (Protein induced by vitamin K absence or antagonist-II /PIVKA_II) Pada HCC : terjadi penurunan aktivitas -glutamyl carboxylase (GGC) tanpa defisiensi vit K, dg abnormal prothrombin time. Defek post-translational yang didapat pada prekursor prothrombin. Pada orang normal prothrombin diproduksi hepatosit ; dg konversi 10 glutamic asid (Glu) residu didekat domain NH2-terminal dari prekursor prothrombin, menjadi -carboxyglutamic acid (Gla) oleh enzim vit K dependent carboxylase dg -carboxylasi.
bile duct cancer Risk factors • Patients with chronic ulcerative colitis who develop primary sclerosing cholangitis are prone to cholangiocarcinoma. The lifetime risk of developing this cancer is 10-20% with primary sclerosing cholangitis. Some patients with Crohn's disease may also be at risk. • Infection with the liver flukes Clonorchis sinensisand Opisthorchis viverrini have been causally linked. Ascaris lumbricoides infection has also been implicated. • Industrial chemical exposure: chemicals used in the aircraft, rubber and wood-finishing industries have been implicated • Thorium exposure is associated with an increase in cases of cholangiocarcinoma.[ • Congenital abnormalities of the bile ducts, eg choledochal cysts. • Caroli's disease (a rare congenital disorder of the intrahepatic bile ducts associated with autosomal recessive polycystic kidney disease where the bile ducts become chronically dilated). • Recently implicated potential risk factors for the intrahepatic form include hepatitis C,HIV, cirrhosis and diabetes.
bile duct cancer The patient usually presents with the following symptoms • jaundice (yellowness of the skin) • poor appetite , Weight loss is variable and weakness and fatigue. • hepatomegaly. • Abdominal pain, right upper quadrant, in advanced disease. • Pale-coloured stools, passage of dark urine, upper gastrointestinal pain (dull ache in the upper right quadrant), weight loss, anorexia and general malaise are common features. • Pruritus • Splenomegaly is present if prolonged biliary obstruction has caused secondary biliary cirrhosis. • The presence of a palpable gallbladder (Courvoisier's sign) may occur with tumours distal to the cystic duct.
Investigations • Diagnosis: radiological investigations (including CT or MRI) and pathological assessment from a biopsy, fine needle aspiration or biliary brush cytology.[2] • LFTs: elevated conjugated bilirubin. Cholestatic picture with markedly elevated alkaline phosphatase, gamma-GT elevated with aminotransferases affected minimally. • Prothrombin time and INR may be prolonged. • Tumour markers: carbohydrate antigen (CA) 19-9 and carcinoembryonic antigen(CEA) tumour markers may be raised (also found in other causes of obstructive jaundice). • Alpha-fetoprotein is not produced by cholangiocarcinoma.
Differential diagnosis • Acute cholecystitis. • Bile duct strictures. • Extrabiliary tumour compressing biliary system. • Biliary adenoma. • Primary biliary cirrhosis. • Primary sclerosing cholangitis. • Ascending cholangitis. • Obstructive choledocholithiasis. • Pancreatic tumours. • Choledochal cysts. • Acute hepatitis.
Complications • The risk of biliary tract sepsis is increased and may cause a deterioration which is amenable to antibiotic therapy. • Secondary biliary cirrhosis occurs in 10-20% of patients.
Prognosis • Progressive deterioration with average survival of 12-18 months from diagnosis. The overall survival rates are low because many patients present with unresectable or metastatic disease. • Even in patients undergoing aggressive surgery, five-year survival rates are 10-40% for cholangiocarcinoma. • Prognosis is much better for those with extrahepatic tumours who are suitable for early surgical intervention. • Intrahepatic lesions carry the worst prognosis.
Types of bile duct tumors Two major types of bile duct tumors are found • Distal bile duct tumors: tumors affecting the bottom half of the bile duct • Klatskin's tumors: Tumors affecting the upper part of the bile duct Unresectable distal bile duct cancer • In patients with advanced distal bile duct cancer that is not surgically removable
Klatskin's tumors • Bile duct cancer of the upper part of the bile duct is also called Klatskin's tumor. • Klatskin's tumors involve the upper part of the bile duct as divides to enter the right and the left parts of the liver. The bile ducts in the liver are called right and left hepatic ducts. • The tumor may involve one or both right and left sides of the hepatic ducts as they enter the liver. The hepatic ducts are closely associated with the blood vessels that supply blood to the liver. • Klatskin’s tumors are closely associated with liver and as they grow invasion into the blood vessels that supply blood to the liver
Treatment of Klatskin's tumor • Complete removal of the tumor is the only effective and potentially curative treatment for cancers of the upper bile duct. Klatskin's tumors are removable if: • Blood supply to one side of the liver is not affected by the tumor: Klatskin’s tumors are closely associated with liver and as they grow invasion into the blood vessels that supply blood to the liver is often found. If the blood supply to one side of the liver is free of tumor then the portion of the liver invaded by the tumor can be removed. • The bile duct to one side of the liver is free of tumor: Unresectable Klatskin's tumor • Klatskin's tumor is unresectable if it invades the blood supply to both sides of the liver and/or the hepatic duct to the both sides of the livertherapy treatments are used. In general these tumors respond poorly to treatment
Signs and symptoms of stomach cancer : • Fatigue • Feeling bloated after eating • Feeling full after eating small amounts of food • Heartburn that is severe and persistent • Indigestion that is severe and unrelenting • Nausea that is persistent and unexplained • Stomach pain • Vomiting that is persistent • Weight loss that is unintentional
GASTRIC CANCER Factors that increase your risk of stomach cancer include: • A diet high in salty and smoked foods • A diet low in fruits and vegetables • Eating foods contaminated with aflatoxin fungus • Pickled foods, the use of refrigeration for preserving foods • Family history of stomach cancer • Infection with Helicobacter pylori • Long-term stomach inflammation (chronic gastritis) • Pernicious anemia • Smoking • Stomach polyps
Causes Stomach cancer • In general, cancer begins when an error (mutation) occurs in a cell's DNA. • The mutation causes the cell to grow and divide at a rapid rate and to continue living when normal cells would die. • The accumulating cancerous cells form a tumor that can invade nearby structures. • And cancer cells can break off from the tumor to spread throughout the body.
It is well known that Helicobacter pylori infection is one of the major risk factors for gastric cancer, And that low values of the pepsinogen (PG) I-to-II ratio can be a marker for atrophy of the gastric mucosa, as well as a marker for gastric cancer risk . Therefore, the prevalence of H. pylori infection and the frequency of gastric mucosal atrophy may influence the incidence of gastric cancer.
FOBT (Fecal Occult Blood Test):* darahtersamaruntukm’deteksiadanyadarah yang tersembunyi (tu. pd usus) Indikasi: Ca Colon /lambung, Adenoma.Colitis ulcerativa.Diverticulitis. Ulcuslambung.Hernia diapragmatika CA19-9* • CA19-9 is a monoclonal antibody generated against a colon carcinoma cell line to detect a monosialogangliosidefound in patients with gastrointestinal adenocarcinoma. • It is found it to be elevated in 21 to 42% of cases of gastric Ca 20 to 40 % of colon Can, & 71 to 93 % of pancreatic Ca. • Has been proposed to differentiate benign from malignant pancreatic disease, but this capability remains to be established.
alpha 4GnT • the quantitative RT-PCR method targeted to alpha 4GnT mRNA will be useful for the detection of circulating gastric cancer cells in the peripheral blood. CA72-4* • more important than CA19-9 as a tumor marker in gastric cancer patients. • The CA 72-4 test recognizes the presence in serum of mucin-like tumour associated glycoprotein TAG 72 (M W 400.000 daltons) • the use of serum CA 72-4 measurements may be more useful than other tumor markers in the diagnosis, prognosis and detection of recurrence in patients with gastric cancer. appeared to be a useful marker for managing gastric cancer. • highly specific to gastric cancer and may be more reliable as a tumour marker than CEA for gastric cancer. • a reliable tumour marker of disease stage and activity in gastric cancer.