Download
1 / 106
1.13k likes | 2.08k Views
PULMONARY TUBERCULOSIS. Definition Chronic inflammatory response of prolonged duration (weeks,months,years) provoked by the persistence of the causative organism Mycobacterium tuberculosis accompanied by tissue destruction and repair of lung tissue.

E N D
Definition Chronic inflammatory response of prolonged duration (weeks,months,years) provoked by the persistence of the causative organism Mycobacterium tuberculosis accompanied by tissue destruction and repair of lung tissue.
Tuberculosis (abbreviated as TB for tubercle bacillus or Tuberculosis) is a common and often deadly infectious disease caused by mycobacteria, mainly Mycobacterium tuberculosis. Tuberculosis usually attacks the lungs (as pulmonary TB). Pulmonary Tuberculosis
TB TransmissionWhat is TB? • TB is a disease caused by infection with a bacteria called Mycobacterium tuberculosis.
Causative organism: Mycobacterium tuberculosis Morphology : • Slender • Aerobic • Weakly Gram + Rod • Grows in straight or branching chains • Unique waxy cell wall • Acid Fast due to MYCOLIC ACID in the cell wall
AFB smear Mycobacterium tuberculosis (stained red) in sputum
Pulmonary Tuberculosis • Scanning electron micrograph of Mycobacterium tuberculosis
Characteristics of Mycobacterial infection • Infiltration of mononuclear cells • Tissue destruction • Healing with scar formation and fibrosis
Other Characteristics: • Mode of transmission – Person to person by air born organisms • Reservoir – Humans with active disease of the lung • Primary infection – Usually asymptomatic • Secondary infection - Reactivation of primary focus • Tissue destruction by inflammatory cells • Attempts at repair with granuloma formation and fibrosis
TB TransmissionHow can you catch TB? • TB is spread through tiny drops sprayed into the air when an infected person coughs, sneezes, or speaks, or another person breathes the air into their lungs containing the TB bacteria.
Epidemiology of Tuberculosis • Affect 1.7 billion people worldwide • 8-10 million new cases every year • 1.6 million deaths every year • Over 10 million people infected with both HIV and M. tuberculosis • 14000 new cases in USA every year
Predisposing factors • Poverty • Overcrowding • Any chronic debilitating illness • Certain disease states: - Diabetes mellitus - Hodgkins lymphoma - Chronic lung disease (esp. silicosis) - Chronic renal failure
Other predisposing conditions: • Malnutrition • Alcoholism • Immunosupression
TB - Infection & DiseaseCategories of TB - Latent & Active • TB disease varies with age and the ability of your body to fight off bacteria. • HIV is the strongest risk factor for the progression of Latent TB to Active TB infection.
Immunology • Delayed hypersensitivity reaction • Mantoux Test : - Intradermal inj. of PPD - Visible/palpable induration >10 mm after 72 hrs - Signifies T-cell mediated immunity to mycobacterial antigen
Diagnostics • Inject intradermally 0.1 mlof 5TU PPD tuberculin • Produce wheal 6 mm to 10mm in diameter • Represent DTH (delayed type hypersensitivity)
Reading of Mantoux test • Read reaction 48-72 hours after injection • Measure only induration • Record reaction in mm
Even if a Skin Test is Negative….. THINKTB! FFever Coughing up Blood Anorexia Chills Chiclls Loss ofAppetite Fatigue Difficulty in Breathing Nightsweats
False negative; certain viral inf., sarcoidosis, malnutrition, hodgkins lymphoma, immunosupression, miliary tuberculosis. • False positive; atypical mycobacterial inf., BCG vaccination
Pathogenesis :The Players (mononuclear phagocyte system) • Macrophages • Scattered all over (microglia, Kupffer cells, sinus histiocytes, alveolar macrophages, etc.) • Circulate as monocytes and reach site of injury within 24 – 48 hrs and transform • Become activated by T cell-derived cytokines, endotoxins, and other products of inflammation
Macrophages serve to eliminate injurious agents and initiate repair- however, they are as well responsible for much of the tissue injury that occurs Tissue macrophage Activated T cell or NK cell Non Immune activation: Endotoxins, fibronectin, chemical mediators IFN-g Activated macrophage Fibrosis (Scaring) Growth factors involved in fibroblast proliferation (PDGF,TGFb,FGF) Angiogenesis factors (FGF,VEGF) Collagen deposition (IL-13 and TGFb) Tissue injury Toxic oxygen metabolites Metallo-proteases Coagulation factors AA metabolites and NO
The Players…. • T and B lymphocytes • Antigen-activated (via macrophages and dendritic cells) • Release macrophage-activating cytokines (in turn, macrophages release lymphocyte-activating cytokines until inflammatory stimulus is removed) • Plasma cells • Terminally differentiated B cells • Produce antibodies
The dominant cellular player in pulmonary tuberculosis is the tissue macrophage Blood monocyte Tissue macrophage (RES) migrate into tissue within 48 hours after injury Kupffer cell (liver) Microglia (CNS) Histiocytes (spleen) Alveolar macs (lung) and differentiate It is joined by lymphocytes and plasma cells, however mast cells and eosinophils are as well involved in chronic allergic diseases Plasma cell Lymphocyte
Pathogenesis • A-Primary Pulmonary Tuberculosis (0-3 weeks): inhalation of Mycobacteria---enter alveolar macrophages---replication in phagosome---bacteremia---seeding of multiple sites
Pathogenesis • B -Primary pulmonarytuberculosis (>3 weeks): Alveolar macrophages---IL-2---T Cells--- T-helper cells---Activated macrophages (i)--- TNF,Chemokines—Hypersensitivity (epith. granulomas) and (ii)---Nitric oxide,reactive O2 sp.---Immunity (bactericidal activity)
Primary Tuberculosis • Develops in unexposed, unsensitized persons • Mostly(95%) asymptomatic; Infection contained • In 5 % symptomatic; Primary progressive tuberculosis • Source of organism; Exogenous • Difficult to diagnose
Primary Tuberculosis Presentation : • Lung consolidation; Lower and middle lobes • Hilar lymphadenopathy • Pleural effusion • In majority organism remain dormant • In severe immunosupression - TB Meningitis - Miliary Tuberculosis
Secondary Tuberculosis • Arises in previously sensitized host • Many years after primary infection • Reactivation of latent infection or overwhelming exogenous infection • Involves apex of upper lobes • Cavitation more prominant
Secondary Tuberculosis • In majority symptomatic; insidious onset of malaise, anorexia, weightloss, fever, productive cough (mucoid, purulent, hemoptysis) , pleuritic pain. • Extrapulmonary manifestations • May be asymptomatic when localised
TB Infection & DiseaseThere are 2 Categories of TB: Latent & Active • TB infection of the lungs can fall into 2 categories of disease: Latent TB or Active TB. • Latent TB means a person is infected by TB bacteria, but cannot infect others, and is not coughing or appearing sick. • Latent TB means the body’s immune system has contained the infection.
TB - Infection & Disease Categories of TB - Latent • Persons with latent TB are identified by a positive skin test (PPD). • Persons who are not infected with Mycobacterium tuberculosis have a negative skin test (PPD).
In Pulmonary Tuberculosis macrophage accumulation persists by different mechanisms: • Continued recruitment of monocytes from the circulation • Local proliferation • Prolonged survival and immobilization
Outcome of Tuberculous infection • Ulcers • Fistulas • Granulomatous diseases • Fibrotic diseases • and combinations of the above
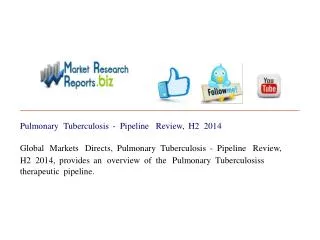
Diagnosis • History • Physical examination • X-Rays ;Consolidation/ cavitation in lung apices • Sputum for AFB : - Z.N Stain - > 10000 organisms in clinical specimen
Diagnosis • Sputum Culture : - conventional ---upto 10 weeks - liquid --- within 2 weeks • P.C.R : - 10 org. in clinical specimen
Chest radiography • No chest X-ray pattern is absolutely typical of TB • 10-15% of culture-positive TB patients not diagnosed by X-ray • 40% of patients diagnosed as having TB on the basis of x-ray alone do not have active TB
Number of sputum samples required • overall diagnostic yield for sputum examination related to • the quantity of sputum (at least 5 mL) • the quality of sputum • multiple samples obtained at different times to the laboratory for processing • 3 samples obtained at least eight hours apart with at least one sample obtained in the early morning
Morphology A-Primary Tuberculosis : • Ghon complex - subpleural parenchymal lesion (lower part of upper lobe) - hilar lymphadenopathy • Progressive fibrosis • Calcification