Download
1 / 90
900 likes | 936 Views
Digestive Drug Agents. Contents. Antacids Histamine 2 blockers Proton pump inhibitors (PPI) Anti-diarroheal drugs Laxatives Anti-emetics. Peptic ulcer. Peptic ulcer occurs in that part of the gastrointestinal tract which is exposed to gastric acid and pepsin.

E N D
Contents • Antacids • Histamine 2 blockers • Proton pump inhibitors (PPI) • Anti-diarroheal drugs • Laxatives • Anti-emetics
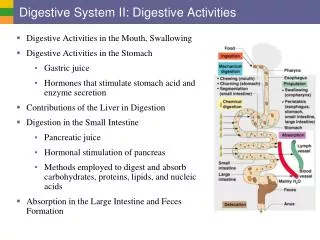
Peptic ulcer • Peptic ulcer occurs in that part of the gastrointestinal tract which is exposed to gastric acid and pepsin. • The etiology of peptic ulcer is not clearly known. It results probably due to an imbalance between the aggressive (acid, pepsin, bile, and H.pylori) and defensive ( gastric mucus, bicarbonate secretion, prostaglandins, and nitric oxide )
Approaches for the treatment PUD • H2-blockers: Cimetidine, ranitidine, Famotidine, and roxitidine • Proton pump inhibitors: Omeprazole, lansoprazole, pantoprazole, rabeprazole, Esomeprazole. • Anticholinergic: Pirenzepine, propantheline, oxyphenonium. • Prostaglandin analogue: misoprostol
Continued • Neutralization of gastric acid • systemic: sodium bicarbonate and sodium citrate • Nonsystemic: mg hydroxide, magnesium trisilicate, aluminum hydroxide gel, and calcium carbonate
Continued • Ulcer protective's: Sucralfate, and bismuth subsalicyte. • Anti-h-pylori drugs: amoxicillin, Clarithromycin, Metronidazole, Tinidazole, and tetracycline.
Antacids • Antacids have been used for centuries in the treatment of patients with acid related disorders. • They were the principle of anti-ulcer treatment until the availability of histamine 2 blockers in the late of 1970s. • The ancient Greece used crushed coral (calcium carbonate)in the first century to treat patients of dyspepsia
Continued • These are basic substances which neutralize gastric acid and raise PH of gastric contents. • Antacids donot decrease acid production, rather agents that raise the antral PH to greater than 4.
Sodium bicarbonate • It is water soluble but the duration of action is short. • It is potent neutralizer, Ph may rise above 7. • It is absorbed systematically, large doses will induce alkalosis • Produces carbon dioxide in stomach, distention, discomfort, belching, risk of ulcer perforation. • Increases sodium load, may worsen edema and CHF.
Continue • However antacids are extensively used, especially on OTC market. • In addition many antacids contain simethicone which reduces gas and bloating. • Basically there are three forms of antacids: • Aluminum antacid • Calcium antacid • Magnesium antacid
Continue • The OTC antacid formulations are available: • Capsules • Tablets • Powders • Chewable tablets • Suspension
Mechanism of action • Antacids originally believed to work by neutralization of gastric acidity. • They donot nothing for prevent over production of acid. • They do this by stimulating: • Mucus • Prostaglandin • Bicarbonate secretion
Drug Effects • The primarily drug effect of antacids is the reduction of the symptoms associated with various acid related disorders such as peptic ulcer disease and hyperacidity. • The ability of antacids to reduce the pain associated with acid related disorders is thought to be result, inhibition of protein digesting ability of pepsin.
Side-Effects • Mg results diarrhea • Al & Ca can result constipation. • Rebound hyperacidity
Aluminum • The amount of antacid necessary to neutralize hydrochloric acid depends on the: • Patient • Condition been treated • Buffering capacity of the preparation used. • Adult dosage is 5-10ml 3-4 times a day, Hs.
Calcium • Calcium carbonate neutralization will produce gas and possible belching, for this reason it may be combined with an anti-flatulent type of drug such as simethicone. • Calcium containing products have a long duration of acid action, which can cause hyperacidity rebound. • Calcium carbonate is available 1-2 tabs Prn.
Magnesium • Mg containing antacids commonly cause a laxative effect and frequent administration of these antacids alone often cannot be tolerated. • Administration of Mg containing antacids is dangerous in patients with renal failure, because of failing of kidney cannot excrete extra Mg and accumulation may occur.
Histamine-2 Blockers • Histamine -2 blockers reduce Hcl but donot abolish stimulated acid secretion. • They have become the most popular drugs for the treatment of many acid related disorders. • These can be attributed by their: • Efficacy • Safety profile • Patient acceptance
Drugs • Cimetidine • Famotidine • Nizatidine • Ranitidine
Mechanism of action • They have ability of blocking parietal cells. • They reduce the amount of Hcl in the parietal cells.
Side-Effects • Confusion • Lethargy • Headache • Abdominal cramp
Cimetidine • In 1977 Cimetidine was the first agent in this class to be released in the market. • Cimetidine comes available 200, 300, 400, 800mg tablets, 300mg/ml, 200mg/ml, 150mg/ml parentral injection.
Proton pump inhibitors (PPI) • PPI is introduced for the treatment of acid related disorders. • The enzyme H+/K+ ATPase is the final common step in acid Secretory processes. • PPI drugs are: • Omeprazole 20mg • Lanzomeprazole 30mg • Esomeprazole 40mg • Pantoprazole 20, 10mg • Rapiprazole 20mg
Mechanism of action • PPI irreversible binds to H+/K+ATPase. The binding of this enzyme prevents the movement of hydrogen ions out of the parietal cell into the stomach, there by blocking all gastric acid secretion. • PPI makes the patient achlorhydric.
Side-effects • Headache • Dizziness • Vomiting • Nausea • Rash • Fatigue
Omeprazole • Omeprazole is a prodrug. • Omeprazole is degraded at low PH and must be given in granules. • Omeprazole inhibits cytochrome P450 system, decreasing metabolism of Warfarin, diazepam, Carbamazepine, and phenytoin and enhancing the effect of these drugs.
Continue • Omeprazole is currently approved only for the acute treatment of severe gastrointestinal reflux disease un responsive to: • Antacids • Antiflatulents • H2-blockers • Adult dosage is 20mg/day for 4-8 weeks.
Ulcer protective agents • Sucralfate: it is compound of aluminum and sucrose which coats the base of the ulcer protecting it from pepsin and acid allowing it to heal. • Dosage is 1gm 1 hour before each meal.
Bismuth Compound • It protects the ulcer by causing coagulation at the base of the ulcer. It has also anti H. pylori action. • It should not be combined with antacids. • The tongue and the stool may appear black after taking dosage 120gm 1 hour before meals and at the bed time.
Prostaglandins • Prostaglandins exert some protective effect on the gastric mucosa and this is why NSAIDs which inhibits prostaglandin synthesis can cause peptic ulceration. • One of the prostaglandin preparation misoprostol reduces the risk of gastric ulcers in patients who are taking NSAIDS, especially in elderly patients having history of ulcers.
Treatment of H. pylori • For helicobacter pylori associated ulcers, there are two therapeutic goals: • Heal the ulcer • Eradication of the organism • The best treatment regimen is for a 10-14 days of Triple Drug regimen.
Continue • The regimen consists of: • PPI, E.g omeprazole 20mg BD • Clarithromycin 500mg BD • Metronidazole 400mg BD
Treatment of NSAIDS associated ulcers • For treatment of aspirin or other NSAIDS induced ulcers the best treatment is to give a proton pump inhibitor, which provides prompt healing of the ulcer. • PPI are also useful in bleeding ulcers as they raise the gastric PH. It is observed that intra gastric PH above 6 may enhance coagulation and platelet aggregation.
Magnesium Case study • ID/CC: A 22 year old female presents to the ER with severe abdominal colic and a history of profuse watery diarrhea of several days duration. • HPI: She also complains dizziness and desire to lose weight, that she has been taken by magnesium sulfate. • PE: Hypotension, lethargy. • Labs: Hypokalemia • Discussion: • Treatment:
Anti-diarrheals Agents • Diarrhea is defined as the abnormal frequent passage of loose stools. • Diarrhea is the abnormal passage of stools with increased frequency, fluidity and weight. • Diarrhea is divided into: • Acute diarrhea • Chronic diarrhea
Causes of Diarrhea • Acute Diarrhea • Bacterial • Drug induced • Viral • Nutritional • Protozoal
Continue • Chronic Diarrhea • Tumors • Diabetes mellitus • Hyperthyroidism • Addison's disease • Irritable bowl syndrome
Anti-diarrhoe Agents • Electrolytes • Bulk agents • Absorbents • Anti-inflammatory • Opioids • Intestinal flora modifiers
Bismthus subsalicyte • Bismuth subsalicte is a pregnancy category C agent. • It should be used with caution in children and teenagers who have or are recovering from chicken pox or flu because of attendance risk of Reyes syndrome.
Continue • Bismuth subsalicyte have two harmless side-effects: • Darkening of the stool • Darkening of the tongue • It is available in a OTC drug. • Available 262 mg chewable tablet and 262 mg/15ml suspension.
Attapulgite • Attapulgite has replaced the use of kaolin-pectin in this preparation. • Kaolin is a naturally hydrated aluminum compound that is now rarely used as an anti-diarrheal agents. • How ever pectin which is extracted from the apples or citrus fruit and is used in many combination products.
Continue • The original kaopectate contained 980mg/5ml of kaolin and 21.7 mg/5ml of pectin. • Attapulgite is an OTC agent. • It is a pregnancy category C agent. • Available 300mg chewable tablet and 600mg/15ml solution.
Diphenoxylate & Atropine (Lomotil) • Lomotil is a synthetic opiate agonist that is structurally related to meperidine. • It has little or no analgesic activity. • It is classified in a pregnancy category C agent. • Available as 2.5mg/5ml + 0.025mg/5ml atropine solution, and 2.5mg + 0.025mg, diphenoxylate and atropine respectively.
Loperamide • Loperamide is a synthetic anti-diarrheal that similar to diphenoxylate. • Decreases the number of stools and water content. • It is the only opiate anti-diarrheal agent that is available as an OTC medication. • Loperamide is a pregnancy category B agent. • Available 1mg tab, 1mg/5ml oral.
Lactobacillus acidophilus • Lactobacillus acidophilus is an acid producing bacteria prepared in a concentrated oral administration. • Has been used for more than 75 years in the treatment of uncomplicated diarrhea, particularly that caused by antibiotic treatment that destroys normal florae.
Continue • It is an OTC medication. • Available 1g powder, 1g tablet, and 1g capsules.
Laxatives • Laxatives are used for the treatment of constipation, which is defined as a condition of abnormally infrequent and difficult passage of feces through the lower GIT. • Constipation is not a disease but it is a symptom of disease.
Causes of Constipation • Pregnancy • Hypothyroidism • Hypokalemia • Parkinsons disease • Iron supplements • Anti-cholinergics • Poor fluid intake
Continue • Lack of exercise • Anxiety • Stress • AL-antacids
Classification of Drugs • Bulk-forming agents • Methylcellulose • Psyllium • Polycarbophil • Stool Softeners- Emollient • Docusate salts • Mineral oil • Glycerin