Download
1 / 40
470 likes | 1.02k Views
Phakic IOL Overview. António Marinho, MD PhD Departamento de Cirurgia Refractiva Hospital Arrábida Porto Portugal. DEFINITION. REFRACTIVE SURGERY To change in a permanent way the refractive power of the eye. How to achieve this goal ?. Change the corneal power (PRK,LASIK)

E N D
Phakic IOL Overview António Marinho, MD PhD Departamento de Cirurgia Refractiva Hospital Arrábida Porto Portugal
DEFINITION • REFRACTIVE SURGERY • To change in a permanent way the refractive power of the eye
How to achieve this goal ? • Change the corneal power (PRK,LASIK) • Change the power of the lens (RLE) • Introduce a new refractive surface (Phakic IOL)
Why Phakic IOLs? Phakic IOL’s are ideal for high ametropias because: • High predictability even in very high ametropias • Stability of refraction • Preserve accomodation • No loss (usually gains) of lines of BSCVA
Myopia - Subjective Refraction under - 7D : LASIK above -7D: Phakic IOL Main Factor : Pachymetry Hyperopia - Cycloplegic Refraction under + 3D : LASIK above + 4D: Phakic IOL Main factor: Keratometry Age Mínimal Age 18 years exceptions anisometropia Stable refraction in the last 18 months Above 50 years low ametropia LASIK high ametropia CLE WHEN PHAKIC IOLs ?
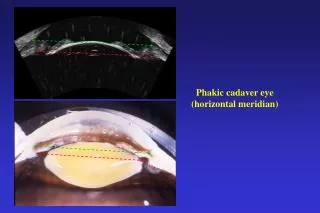
INCLUSION CRITERIASpecific • Anterior chamber anatomy (AC depth and AC size) • Endothelium profile • Iris shape Pupil Size • Perfect Surgery
Bad Selection • Endothelial Decompensation • Shallow AC
Endothelium Profile • Endothelial cell count: • 21 to 25 years 2800 cells/mm • 26 to 30 years 2650 cells/mm • 31 to 35 years 2400 cells/mm • 36 to 45 years 2200 cells/mm • > 45 years 2000 cells/mm • Endothelial cell shape (avoid high polymagatism)
Endothelial Cell Count • Before Surgery (inclusion criteria) • 3 months after (shows surgical trauma) • Yearly afterwards (if important decrease EXPLANT)
ACRYSOF • Hydrophpbic Acrylic IOL • 4 point angle fixation • 6.0 mm Optic • -6.00/-16.50 • 4 sizes (12.5,13.0,13.5 and 14.0mm)
Acrysof Surgery • Introduce the IOL in the cartridge (diving position) • 2.6 mm incision • Inject the IOL into the eye (past pupil) • NO iridectomy • No suture
ANGLE SUPPORTED AC PIOLs • Angle to angle distance very important • Size of the IOL is critical • Contact with the angle and iris root • May be close to endothelium • Far away from lens
ARTISAN 5.0mm • Iris-Claw phakic IOL • PMMA • 5.0 mm O.Z. • Available for myopia, hyperopia (-23.00 to +12.00) and astigmatism( +/-)
ARTISAN 6.0mm • Iris-Claw phakic IOL • PMMA • 6.0 mm O.Z. • Available for myopia (-2.00 to –15.00)
Artisan Surgery • 2 side ports • Main incision • Fill AC with visco • Introduce and rotate the IOL • Enclavation of iris tissue • Iridectomy • Suture
ARTIFLEX • Iris-claw phakic IOL • PMMA haptics • Silicone (foldable optic) • 6.00mm • One size fits all
TORIC ARTIFLEX • Myopia -1.00 to -14.50 • Cylinder -1.00 to -7.50 • Two models (axis at 180º and 90º) • Sphere + Cylinder < -14.50
ARTIFLEX • 2 side ports • Main incision (3.2mm) • Fill AC with visco • Introduce and rotate the IOL • Enclavation of iris tissue • Iridectomy • No Suture
IRIS SUPPORTED PIOLs • One size fits all • No angle touch • Close contact with the iris (grasp) • Safe distance from the endothelium • Far away from the lens
Not Perfect Surgery…. • Decentration is always a surgeon’s fault • These lenses are always centered regardless of the pupil • Luxation of the IOL(traumatic or spontaneous)is due to weak grasp
Bad Selection • Posterior Synaechia • Convex Iris • Shallow AC
IOL DEPOSITS • Rare • Disappear spontaneouly after 3 months in most cases • May need steroid treatment (exceptionally) • Related to surgical manipulation
ICL V4c • The NEW ICL V4 c has a tiny central hole in the middle of the optic • NO iridectomy is needed
ICL Surgery • Load the ICL in the cartridge • 2 side ports (12 and 6) • Main incision (temporal) • Introduce IOL in AC • Place IOL behind the iris • Constricit the pupil • Iridectomy (if not YAG before)
Posterior Chamber PIOLs • Sit on sulcus (ICL) or “float” in aquous humour (PRL) • “Vault” (the space between ICL and lens) is crucial and depends on the IOL size • Close contact with the lens • Very far away from the endothelium
Size matters….. • Short ICL: Decentration and small vault • Long IOL: Excessive vault
If there is no vault… • Anterior subcapsular cataract (less frequent as the surgical technique and sizing devices get better)
Refractive ResultsBCVA>20/40 • Artisan 93.9% (518 eyes) • ICL 94.7% (331 eyes) • Cachet 100% (113 eyes)
Refractive Results Safety • PIOL GAIN LOSS • Artisan 43.5 % 1.2% • ICL 40.6% 0% • Cachet 27.3% 0%
Refractive ResultsConclusions • All Phakic IOLs have GREAT refractive results • Most eyes gain lines • The KEY to select a phakic IOL are not the refractive results ,but the complications