Download
1 / 216
2.23k likes | 2.91k Views
Mechanics of respiration. Dr.Kalpana B. The Respiratory System. The Mechanics of Breathing. VENTILATION. Breathing in – inspiration / inhalation Breathing out – expiration / exhalation. Inspiration uses external intercostals and diaphragm

E N D
Mechanics of respiration Dr.Kalpana B
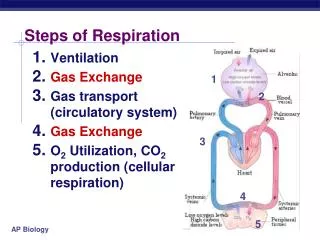
The Respiratory System The Mechanics of Breathing Mechanics of Breathing
VENTILATION • Breathing in – inspiration / inhalation • Breathing out – expiration / exhalation
Inspiration uses external intercostals and diaphragm • Accessory muscles of respiration:scalenes, sternocleidomastoid, pectoralis minor Work during forced inspiration, exercise, airway obstruction.
MUSCLES OF INSPIRATION • Diaphragm - increases the vertical diameter of chest wall • External intercostals - increase the transverse and A-P diameters of chest wall
Expiration is passive at rest, results from elastic recoil of chest wall and lung • But uses internal intercostals and abdominal muscles during forced expiration. • Breathing rate is 10-20 breaths / minute at rest, 40 - 45 at maximum exercise in adults
ACCESSORY MUSCLES OF INSPIRATION • Sternocleidomastoid • Scaleni • Pectoralis minor ( Work during forced inspiration, exercise, airway obstruction)
EXPIRATION • Passive process • Results from elastic recoil of chest wall and lungs
MUSCLES OF FORCED EXPIRATION • Abdominal recti, transversus abdominis, obliques. • Internal intercostals
Internal intercostal muscle Abdominals
Movement of the Diaphragm Figure 17-9b
Movement of the Rib Cage during Inspiration Figure 17-10a
Movement of the Rib Cage during Inspiration Figure 17-10b
Inspiration • Inspiration-Active process • More volume -> lowered pressure -> air in. (Negative pressure breathing.) • Intrapulmonary pressure decreases (758 mm Hg
Pressures That Cause the Movement of Air In and Out of the Lungs(Pressure changes during ventilation)
Pleural Cavity Very small space Maintained at negative pressure Transmits pressure changes Allows lung and ribs to slide Lungs Gas Exchange Chest Wall (muscle, ribs) Diaphragm (muscle) Pleural CavityImaginary Space between Lungs and chest wall
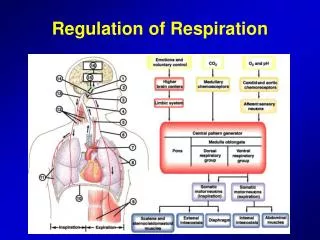
Pressure Relationships in the Thoracic Cavity • Respiratory pressure is always described relative to atmospheric pressure • Atmospheric pressure (Patm) - pressure exerted by the air surrounding the body • Intrapulmonary pressure (Ppul) – pressure within the alveoli • Intrapleural pressure (Pip) – pressure within the pleural cavity
Intra pulmonary pressure/ alveolar pressure: pressure in the pleural space Expiration -+1mm Hg Inspiration -1 mm Hg Intrapleural pressure pressure in the pleural space Expiration -2.5 to -4 mm Hg Inspiration -6 mm Hg Transmural pressure: pressure difference across the lung
TRANSMURAL PRESSURE • TRANSPULMONARY PRESSURE • The difference between the alveolar pressure and the pleural pressure. • TRANSAIRWAY PRESSURE • Difference between airway and pleural pressure.
Injury to the Chest Wall • Pneumothorax: • allows air into pleural cavity • Atelectasis: • also called a collapsed lung • result of pneumothorax
Pressure in the Pleural Cavity Pneumothorax results in collapsed lung that can not function normally Figure 17-12b
Inspiration • Contraction of diaphragm • Expansion of thoracic cage • Intrapleural ressure becomes more negative • Increased transpulmonary pressure • Inflation of lung • Decreased alveolar pressure which becomes sub atmospheric • Airflows into airway and lungs • Cessation of contraction of inspiratory muscles ends inspiration
Expiration • Relaxation of inspiratory muscles • Dropping of rib cage • Intrapleural ressure becomes less negative • Decrease transpulmonary pressure • Deflation of lung • Increased alveolar pressure which becomes more than atmospheric ressure • Airflows pushed out of lungs • Expiration continues till alveolar pressure equals atmospheric pressure.
Type I Type II
SURFACE TENSION AIR LIQUID
Type I cell Type II cell
Surfactant • Dipalmitoylphosphatidylcholine • Protein-lipid complex • Secreted by type II pneumocytes • Present in the alveolar fluid • Prevents the alveoli from collapsing
Significance of surfactant • Decreases Surface tension • Helps in stability of alveoli of unequal size • Prevent collapse of alveoli during expiration • Prevent bursting of alveoli during inspiration
Keeps the alveoli dry (prevent pul. Congestion) Pulmonary capillary hydrostatic pressure is 8-10 mm Hg Oncotic pressure is 25 mmHg. Inwardly directed pressure gradient. • Helps prevent pulmonary edema
Decreases work of breathing • Role in defense within the lungs against infection and inflammation (SP-A, SP-D) • Promote phagocytosis of bacteria and viruses by alveolar macrophage.
Laplace’s law • Pressure = 2 × tension Radius
Respiratory distress syndrome • Occurs in premature infants(born before 7 completed months) • Deficiency of surfactant • Alveoli collapse after the first breath • Baby goes to severe respiratory distress
Clinical significance of surfactant • (Infant) Respiratory distress syndrome (IRDS) or • Hyaline membrane disease (due to deficiency of surfactant in fetal life) - Administration of phospholipid alone by inhalation - Administration of bovine surfactant (phospholipid and protein)
COMPLIANCE • Compliance is the measure of stretchability or elasticity or distensibility • Compliance is change in volume by unit change in pressure (∆V/∆P) –ml/cm H2O (L/cm H2O)
Types of compliances • As both lungs & thoracic cage has elastic nature –in the respiratory system the various compliances are; • Lung compliance (L.C) • Thoracic compliance (Th.C) • Total compliance (T.C) -- (both L.C & Th.C)
Normal value Compliance in relation to intra alveolar pressure Compliance of lungs and thorax 130ml / 1cm H2O pressure Compliance of lungs alone 0.22l when airway pressure is increased by 1cmH2O then lung expands by 0.22l • compliance of lung alone is 2 times compliance of lung and thorax.
Difference between inflation and deflation pressure volume curve is called hysterics. • The characteristics of the compliance diagram are determined by the elastic forces of the lungs. • (1) elastic forces of the lung tissue and • (2) surface tension of the fluid that lines the inside walls of the alveoli
Factors affecting lung compliance: 1. Distensibility and elastic recoil 2. Lung volume 3. Lung size 4. Surface tension inside alveoli
Specific compliance – It is the compliance per unit volume • Compliance/FRC (in L per cm H2O per L)
WORK OF BREATHING • Under resting conditions, the respiratory muscles normally perform work to cause inspiration but not to cause expiration. • The work of inspiration can be divided into three fractions: (1) Elastic work (65%) (2) Tissue resistance work (7%) (3) Airway resistance work (28%).
Airway resistance The resistance offered to the passage of air through the respiratory tract