Download
1 / 4
40 likes | 112 Views
ntroduction: With easy availability of ultrasound screening and improvement in expertise, hydronephrosis is now a very frequently diagnosed problem reported in 1 to 5% of all pregnancies. This has enabled us to have a better understanding of the natural course of the problem and early intervention before it results in permanent renal damage. The distinction &hellip

E N D
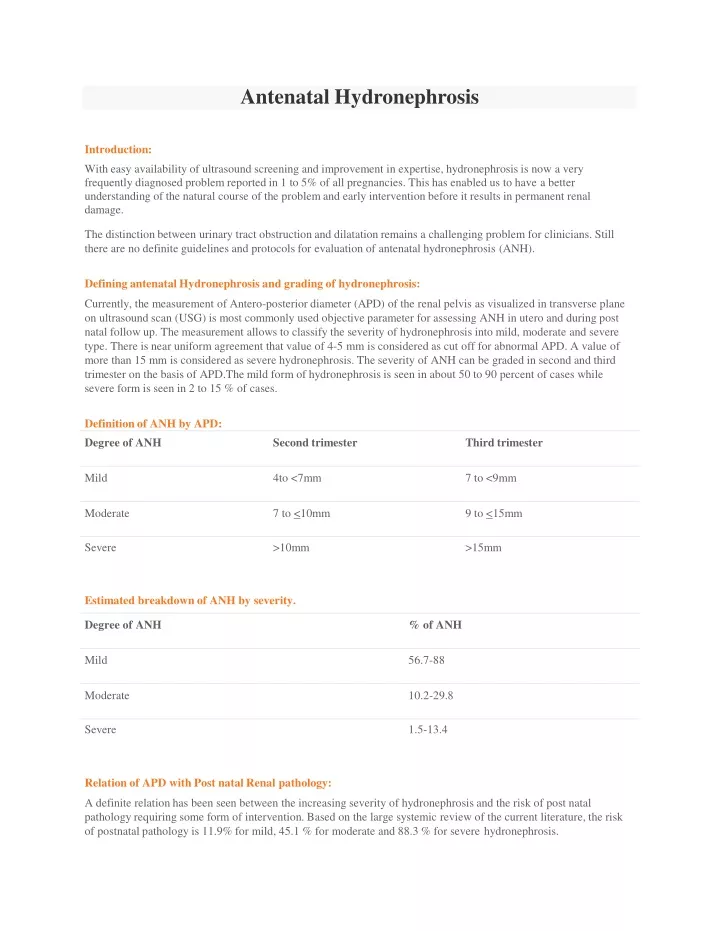
AntenatalHydronephrosis Introduction: With easy availability of ultrasound screening and improvement in expertise, hydronephrosis is now a very frequently diagnosed problem reported in 1 to 5% of all pregnancies. This has enabled us to have a better understanding of the natural course of the problem and early intervention before it results in permanent renal damage. The distinction between urinary tract obstruction and dilatation remains a challenging problem for clinicians. Still there are no definite guidelines and protocols for evaluation of antenatal hydronephrosis(ANH). Defining antenatal Hydronephrosis and grading ofhydronephrosis: Currently, the measurement of Antero-posterior diameter (APD) of the renal pelvis as visualized in transverse plane on ultrasound scan (USG) is most commonly used objective parameter for assessing ANH in utero and during post natal follow up. The measurement allows to classify the severity of hydronephrosis into mild, moderate and severe type. There is near uniform agreement that value of 4-5 mm is considered as cut off for abnormal APD. A value of more than 15 mm is considered as severe hydronephrosis. The severity of ANH can be graded in second and third trimester on the basis of APD.The mild form of hydronephrosis is seen in about 50 to 90 percent of cases while severe form is seen in 2 to 15 % ofcases. Definition of ANH byAPD: Estimated breakdown of ANH byseverity. Relation of APD with Post natal Renalpathology: A definite relation has been seen between the increasing severity of hydronephrosis and the risk of post natal pathology requiring some form of intervention. Based on the large systemic review of the current literature, the risk of postnatal pathology is 11.9% for mild, 45.1 % for moderate and 88.3 % for severehydronephrosis.
Etiology of Antenatal Hydronephrosis: Most children with antenatal history of renal pelvis dilatation ultimately resolve their hydronephrosis. The etiology of this finding may be related to a narrowing of ureteropelvic junction (UPJ) or natural kinks and folds that occur early in development that resolve as the patient matures. The differentiation between transient hydronephrosis versus clinically significant UPJ obstruction remains one of the most controversial challenges in modern pediatric urology. Nevertheless the incidence of transient hydronephrosis ranges from 41 to 88%. Most children with a pelvic dilatation less than 6mm diagnosed during the 2nd trimester or less than 8 mm diagnosed during the 3rd trimester have transienthydronephrosis. Transient Hydronephrosis: Majority of the children with history of ANH will show improvement. The etiology of this finding may be related to a narrowing of the uretero-pelvic junction (UPJ) or natural kinks and folds that occur early in development that resolve as the patient matures. The differentiation of transient hydronephrosis from pathological hydronephrosis is always a clinical challenge. The incidence will vary from 41 to88%. Most children with pelvic dilatation of less than 6 mm diagnosed during the 2nd trimester or less than 8 mm diagnosed during 3rd trimester have transient hydronephrosis. In contrast, the incidence of transient hydronephrosis is only 40% in children with an APD less than 10-12mm detected during the 3rdtrimester. Uretero Pelvic JunctionObstruction(UPJ): Dilatation of pelvi-calyceal system without ureteral dilatation should raise the suspicion of UPJ obstruction. These are the patients with moderate to severe hydronephrosis which will show deterioration on USG and renal scans and then require surgical intervention. The challenge is to pick up the problem and intervene early before it causes permanent renalimpairment. VesicouretericReflux(VUR): The finding of variable dilatation on USG and the presence of hydroureter should the suspicion of VUR.Especially infants with UTI and older children with recurrent UTI should be investigated to rule out the possibility ofVUR. Ureterovesical junction obstruction/Megaureters This is a problem associated with grossly dilated ureters but most of these (72%) will resolve on follow up. MCU study will rule the possibility of reflux in thesecases. Posterior Urethral Valve: The findings of bilateral hydronephrosis, dilated ureters, thickened dilated bladder that fails to empty and dilated posterior urethra on antenatal scan should raise the suspicion of posterior urethral valves. This is a problem which can have high morbidity and poor prognosis depending on the severity of renal damage. One should have very high suspicion of this problem, so that earliest intervention to relieve the obstruction can bedone. Prenatal Evaluation ofANH: The evaluation will depend on the gestational age, severity of dilatation, bilaterality, dilatation of ureter, amniotic fluid index and suspicion of posterior urethralvalve. The suspicion of posterior urethral valve warrants monitoring throughout the pregnancy. In such cases, in the presence of oligohydramnios fetal interventions such as vesicoamniotic shunt may beoffered. Imaging Modalities in evaluation of ANH: Renal/Bladder Ultrasound:
This is most commonly used modality because of its easy availability and absence of radiation.It gives god anatomical details and is used to monitor the parenchymal status and the status of dilatation duringfollow up. Its limitation being it does not give objective information about the functional status of kidney and is a poor independent predictor of those patients that will need surgicalintervention. VoidingCystourethrogram(VCUG): This test gives you information about the lower urinary tract and is important to rule out vesicoureteric reflux and posterior urethral valve. It is usually indicated in moderate to severe hydronephrosis, mild hydronephrosis with recurrent UTI, presence of hydroureter and suspected posterior urethralvalve. Renalscintigraphy: Dynamic renal scintigraphy or DTPA scan is performed to assess the differential functions and to know the severity and level of obstruction. It is usually performed after 6 wks to allow for renalmaturity. Differential function <40% with impaired renal drainage (with T1/2 > 20min) or worsening renal function is often the indication of pyeloplasty. Also it is useful for follow up and post surgicalassessment. Post natal Evaluation ofANH: Post natal evaluation requires detailed work up especially in case of moderate to severe hydronephrosis, hydroureter and in case with suspected posterior urethral valve. The aim of imaging should be to identify the underlying cause of dilatation, differentiate from transient hydronephrosis, to estimate the renal functions and to take decision regarding intervention. The post natal evaluation begins with an ultrasound KUB, usually done after 48-72 hrs except in cases where posterior urethral valve is suspected or there is presence of bilateral hydronephrosis or hydronephrosis in a solitary kidney. The patients with moderate to severe hydronephrosis, hydroureter, posterior urethral valve should be started on prophylactic antibiotics. In cases of posterior urethral valve the complete evaluation and treatment needs to be done beforedischrge. The patients with mild hydronephrosis can be judtfollowed with serial ultrasounds. These patients usually donot require chemoprophylaxis and renal scintigraphy and are only evaulated further in case of increasing dilatation or recurrent UTI’s.DTPA/MAG3 scan is done after 45 days of life and when everPelviureteric junction obstruction is suspected. DMSA scan is performed once a diagnosis of vesico-ureteric reflux and posterior urethral valve is made. Depending on the clinical, renal scintigraphy can be repeated as and when required.The patients with isolated hydronephrosis and retained renal function require long term follow up, although appropriate length of surveillance is yet to be determined. The following chart depicts the algorithm for the management of antenatalhydronephrosis. Antenatal Hydronephrosis Post Natal USG at 48 – 72hrs
Tags = hydronephrosis in child treatment delhi, best pediatric urologist in delhi, best pediatric urologist in india,