Download
1 / 1
10 likes | 114 Views
THE NUTS, BOLTS, AND RESULTS OF MULTI-SITE PROJECTS Helen N. Turner, DNP, RN-BC, PCNS-BC, Pediatric Pain Management Center, Doernbecher Children’s Hospital, OHSU, Portland, OR

E N D
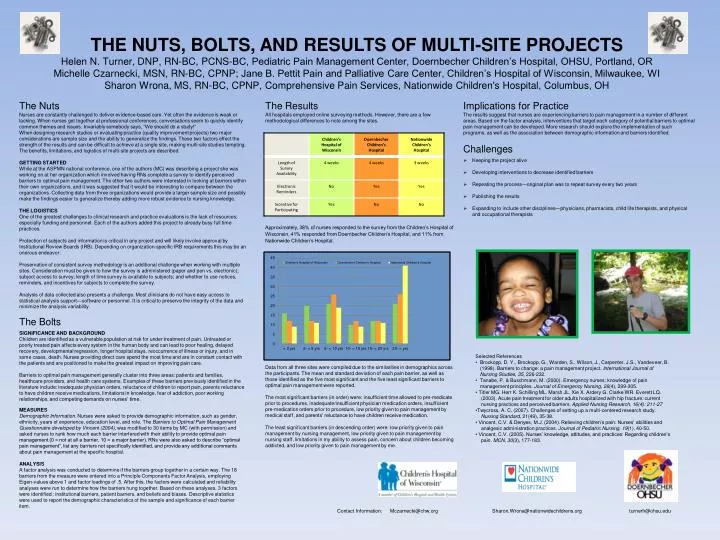
THE NUTS, BOLTS, AND RESULTS OF MULTI-SITE PROJECTS Helen N. Turner, DNP, RN-BC, PCNS-BC, Pediatric Pain Management Center, Doernbecher Children’s Hospital, OHSU, Portland, OR Michelle Czarnecki, MSN, RN-BC, CPNP; Jane B. Pettit Pain and Palliative Care Center, Children’s Hospital of Wisconsin, Milwaukee, WI Sharon Wrona, MS, RN-BC, CPNP, Comprehensive Pain Services, Nationwide Children's Hospital, Columbus, OH The Nuts Nurses are constantly challenged to deliver evidence-based care. Yet often the evidence is weak or lacking. When nurses get together at professional conferences, conversations seem to quickly identify common themes and issues. Invariably somebody says, “We should do a study!” When designing research studies or evaluating practice (quality improvement projects) two major considerations are sample size and the ability to generalize the findings. These two factors effect the strength of the results and can be difficult to achieve at a single site, making multi-site studies tempting. The benefits, limitations, and logistics of multi-site projects are described. GETTING STARTED While at the ASPMN national conference, one of the authors (MC) was describing a project she was working on at her organization which involved having RNs complete a survey to identify perceived barriers to optimal pain management. The other two authors were interested in looking at barriers within their own organizations, and it was suggested that it would be interesting to compare between the organizations. Collecting data from three organizations would provide a larger sample size and possibly make the findings easier to generalize thereby adding more robust evidence to nursing knowledge. THE LOGISTICS One of the greatest challenges to clinical research and practice evaluations is the lack of resources; especially funding and personnel. Each of the authors added this project to already busy full time practices. Protection of subjects and information is critical in any project and will likely involve approval by Institutional Review Boards (IRB). Depending on organization-specific IRB requirements this may be an onerous endeavor. Preservation of consistent survey methodology is an additional challenge when working with multiple sites. Consideration must be given to how the survey is administered (paper and pen vs. electronic); subject access to survey; length of time survey is available to subjects; and whether to use notices, reminders, and incentives for subjects to complete the survey. Analysis of data collected also presents a challenge. Most clinicians do not have easy access to statistical analysis support—software or personnel. It is critical to preserve the integrity of the data and minimize the analysis variability. The Results All hospitals employed online surveying methods. However, there are a few methodological differences to note among the sites. Approximately, 38% of nurses responded to the survey from the Children’s Hospital of Wisconsin, 41% responded from Doernbecher Children’s Hospital, and 11% from Nationwide Children’s Hospital. Data from all three sites were compiled due to the similarities in demographics across the participants. The mean and standard deviation of each pain barrier, as well as those identified as the five most significant and the five least significant barriers to optimal pain management were reported. The most significant barriers (in order) were: insufficient time allowed to pre-medicate prior to procedures, inadequate/insufficient physician medication orders, insufficient pre-medication orders prior to procedure, low priority given to pain management by medical staff, and parents’ reluctance to have children receive medication. The least significant barriers (in descending order) were: low priority given to pain management by nursing management, low priority given to pain management by nursing staff, limitations in my ability to assess pain, concern about children becoming addicted, and low priority given to pain management by me. • Implications for Practice • The results suggest that nurses are experiencing barriers to pain management in a number of different areas. Based on the factor analysis, interventions that target each category of potential barriers to optimal pain management can be developed. More research should explore the implementation of such programs, as well as the association between demographic information and barriers identified. • Challenges • Keeping the project alive • Developing interventions to decrease identified barriers • Repeating the process—original plan was to repeat survey every two years • Publishing the results • Expanding to include other disciplines—physicians, pharmacists, child life therapists, and physical and occupational therapists The Bolts SIGNIFICANCE AND BACKGROUND Children are identified as a vulnerable population at risk for under treatment of pain. Untreated or poorly treated pain affects every system in the human body and can lead to poor healing, delayed recovery, developmental regression, longer hospital stays, reoccurrence of illness or injury, and in some cases, death. Nurses providing direct care spend the most time and are in constant contact with the patients and are positioned to make the greatest impact on improving pain care. Barriers to optimal pain management generally cluster into three areas: patients and families, healthcare providers, and health care systems. Examples of these barriers previously identified in the literature include: inadequate physician orders, reluctance of children to report pain, parents reluctance to have children receive medications, limitations in knowledge, fear of addiction, poor working relationships, and competing demands on nurses’ time. MEASURES Demographic Information. Nurses were asked to provide demographic information, such as gender, ethnicity, years of experience, education level, and role. The Barriers to Optimal Pain Management Questionnaire developed by Vincent (2004), was modified to 30 items by MC (with permission) and asked nurses to rank how much each barrier interfered with their ability to provide optimal pain management (0 = not at all a barrier, 10 = a major barrier). RNs were also asked to describe “optimal pain management”, list any barriers not specifically identified, and provide any additional comments about pain management at the specific hospital. ANALYSIS A factor analysis was conducted to determine if the barriers group together in a certain way. The 18 barriers from the measure were entered into a Principle Components Factor Analysis, employing Eigen-values above 1 and factor loadings of .5. After this, the factors were calculated and reliability analyses were run to determine how the barriers hung together. Based on these analyses, 3 factors were identified : institutional barriers, patient barriers, and beliefs and biases. Descriptive statistics were used to report the demographic characteristics of the sample and significance of each barrier item. • Selected References • Brockopp, D. Y., Brockopp, G., Warden, S., Wilson, J., Carpenter, J.S., Vandeveer, B. (1998). Barriers to change: a pain management project. International Journal of Nursing Studies, 35, 226-232. • Tanabe, P. & Buschmann, M. (2000). Emergency nurses; knowledge of pain management principles. Journal of Emergency Nursing, 26(4), 299-305. • Titler MG. Herr K. Schilling ML. Marsh JL. Xie X. Ardery G. Clarke WR. Everett LQ. (2003). Acute pain treatment for older adults hospitalized with hip fracture: current nursing practices and perceived barriers. Applied Nursing Research, 16(4): 211-27 • Twycross, A. C. (2007). Challenges of setting up a multi-centered research study. Nursing Standard, 21(49), 35-38. • Vincent, C.V. & Denyes, M.J. (2004). Relieving children’s pain: Nurses’ abilities and analgesic administration practices. Journal of Pediatric Nursing, 19(1), 40-50. • Vincent, C.V. (2005). Nurses’ knowledge, attitudes, and practices: Regarding children’s pain. MCN, 30(3), 177-183. Contact Information: Mczarnecki@chw.org Sharon.Wrona@nationwidechildrens.org turnerh@ohsu.edu