Download
1 / 13
130 likes | 268 Views
Possible solution: Change testing & care for patients in TB treatment. Old system. New system. TB patient treated at TB center. TB patient treated at TB center. Referred to VCT center for HIV testing. “Opt-out” HIV testing at TB center Rotating VCT counselors TB nurses. If HIV+. If HIV+.

E N D
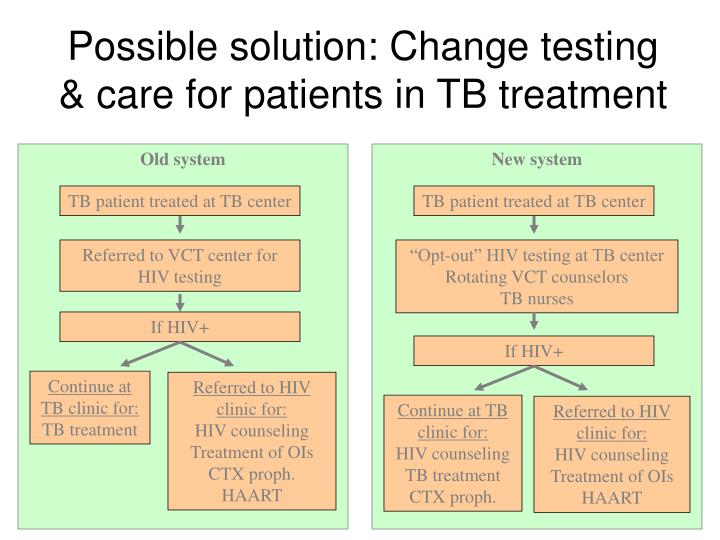
Possible solution: Change testing & care for patients in TB treatment Old system New system TB patient treated at TB center TB patient treated at TB center Referred to VCT center for HIV testing “Opt-out” HIV testing at TB center Rotating VCT counselors TB nurses If HIV+ If HIV+ Continue at TB clinic for: TB treatment Referred to HIV clinic for: HIV counseling Treatment of OIs CTX proph. HAART Continue at TB clinic for: HIV counseling TB treatment CTX proph. Referred to HIV clinic for: HIV counseling Treatment of OIs HAART
How to improve referral? • Better counseling? • Streamline treatment of TB patients at HIV clinic? • Decentralize more HIV services to TB sites? • CD4 counts • HAART
Summary • Current ART’s effective but further innovation of dose, safety and efficacy desirable • Drug development costs in HIV rising • Developing world concentration of epidemic presents unique challenges • Clinical Trial Conduct • Regulatory • Distribution and Access • Pharmacovigilance • Learning from PPP’s to address challenges
HAART in pregnancy... • Is effective and the results are independent from the setting of delivery • Makes possible the breastfeading • Present a very limited life-threatening risk and the hepatic toxicity seems, in a large cohort, to be limited
HAART in pregnancy... • Is well accepted by the patients: 80% of the invited women completed the protocol • Is associated with a decreased rate of viral resistance compared with single dose nevirapine • Is cost-effective
Concluding remarks • Adherence and preventive behaviours are inadequate • No clear association between individual factors and adherence • Decreasing adherence over time: • second year of treatment “high risk” for non-adherence • Implications for antiretroviral resistance • Need for prospective studies of adherence to treatment AND prevention
Public Health Approach to Treatment • Utilize 1st line regimens with predictable mutations and “dead end mutational pattern” • Utilize 1st line regimens which allow for rational 2nd line therapies • Be willing to change 1st line therapeutic approach based on resistance data despite costs • Invest more heavily on community treatment support/adherence programs to ensure high level initial adherence
Conclusion Some of the ART program related risks are real, we need to do much more in moving on the options to mitigate against them Many of the ART program related benefits are real and substantial, we need to do much more on the options to optimize them
Next steps • Study impacts on adherence and treatment outcomes of: • Impact of out-of-pocket expenses and transportation costs (w. household data) • Type of facility and service quality • Other variables … • Similar work in Ghana, Mozambique, Rwanda, South Africa and Kenya
Ingredients of a successfulAIDS Transition • A “Learning Agenda” will help accomplish the AIDS transition • Understand the health & non health benefits of treatment in each country • Understand all the determinants of treatment success in each country • Financing problem: Lower costs, increase effectiveness or increase funding? • Prevention, prevention, prevention
CONCLUSION • TAP has contributed at the national level to the greater involvement of PLWHI elegible for ARV treatment. • TAP has increase an honest collaboration between public health facilities and NGOs. • There is a need to be cautious while implementing resistance sentinel sites of HIV/AIDS and ART. • ART is a essential in Burkina Faso and needs to be continued.
Conclusion • FHI under TAP has engaged the private sector to demonstrate its complementary role to the public sector in ART roll out in Ghana • The pro-poor approach of TAP brings in an element of equity since it can target both the rich and the poor • TAP has demonstrated that quality standards of HIV care and treatment can be assured by the private sector through constant engagement Q: AFTER TAP WHAT NEXT?
Key Lessons • Good ownership & empowerment with performance based financing approach; enhanced accountability and performance • Importance of impact evaluation (i.e. measuring performance contracting; impact of treatment on prevention) • Desire for quick results led to more centralized & vertical approaches at outset; shift towards integration essential at this stage of program • Important potential impact of AIDS investments in terms of work environment (staff recruitment and training, laboratory upgrading, facility rehabilitation, and logistical support)