Download
1 / 31
310 likes | 754 Views
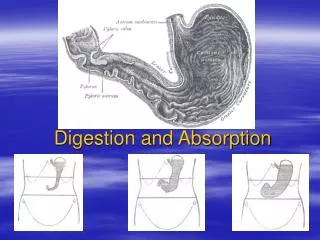
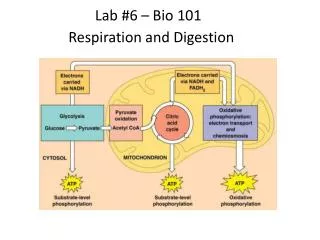
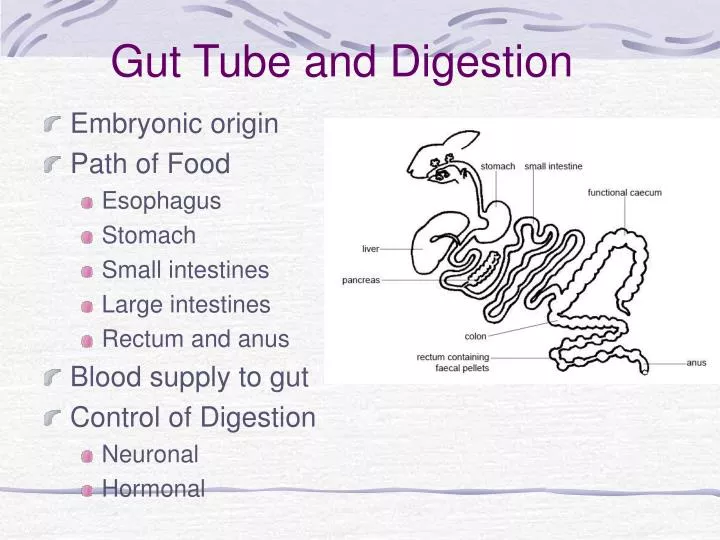
Gut Tube and Digestion. Embryonic origin Path of Food Esophagus Stomach Small intestines Large intestines Rectum and anus Blood supply to gut Control of Digestion Neuronal Hormonal. Mouth--chewing. Path of Food. Pharynx--conscious swallowing. Esophagus--transport to stomach.

E N D
Gut Tube and Digestion • Embryonic origin • Path of Food • Esophagus • Stomach • Small intestines • Large intestines • Rectum and anus • Blood supply to gut • Control of Digestion • Neuronal • Hormonal
Mouth--chewing Path of Food Pharynx--conscious swallowing Esophagus--transport to stomach Stomach--mechanical and chemical breakdown Small Intestines-- chemical digestion and absorption Large Intestines-- resorb water, form feces Rectum---collect and expel feces
Esophagus • Pharynx to stomach • Smooth muscle (conscious swallowing is in pharynx) • Passes through esophageal hiatus in diaphragm, stomach against inferior diaphragm • Cardiac orifice, with esophageal hiatus guard opening to stomach, prevent regurgitation • GERD--gastroesophageal reflux disease • Sometimes due to hiatal hernia • Lower esophagus becomes ulcerous and precancerous • Treat with antacids and other acid-reducing drugs
Histological Layers of Digestive Tract Wall • Three layers generally present—details vary with each organ • Internal Layer = Mucosa • Epithelium • Lamina propria • Muscularis mucosae • Middle Layer = Submucosa • CT w/ elastic fibers, nerves, vessels • Outer Layer = Muscularis Externa (two sub-layers) • circular (“sphinchter” is more internal sub-layer) • longitudinal (more external sub-layer)
Stomach • STRUCTURE • J-shaped but varies from “steerhorn” (high and horizontal) to vertically elongate (down to pelvis on tall, thin people) • From esophagus (cardiac orifice) to small intestine (pyloric sphincter) • Greater, lesser curvatures • FUNCTION • Mechanical breakdown of food--smooth muscle in wall • Protein breakdown--pepsin secreted by epithelial lining • Acidic conditions--for pepsin to work and to kill bacteria • Absorption of water, ions and some drugs (e.g., aspirin, alcohol)
Histology of Stomach • Mucosa • Rugae: mucosal folds allow expansion • Typical Submucosa • Muscularis externa • Oblique layer • Circular layer • Pyloric sphincter • Longitudinal layer • Serosa
Gastric Glands • Gastric glands, in lamina propia, secrete digestive enzymes into fundus of stomach via gastric pits. • 1500 ml of gastric juice per day is pproduced • Parietal cells (proximal in gland) secrete • Intrinsic Factor that facilitates absorption of Vitamin B • HCl components • Chief cells (distal in gland) secrete • Pepsinogen (pepsin precursor) • Rennin in newborns (coagulates milk…used in cheese-making) • Gastric lipase (begins digestion of milk fats)
Fig. 24-13 Fig. 24-14 Fig
When to keep food in stomach or send on: pyloric glands • In pyloric region, modified gastric glands secrete hormones • Secrete mucous • Gastrin—which stimulates other gastric glands and also contractions of smooth muscle (when neural/hormonal stimuli over-ride effect of somatostatin) • Somatostatin—inhibits gastrin (continuously released)
No absorption of nutrients in stomach • Alcohol and other lipid-soluble drugs can be absorbed by penetrating epithelial bi-lipid cell membranes
Small Intestines • Duodenum • C-shaped initial piece (5% of total) • Entries for pancreatic, bile ducts • Jejunum • Fan-shaped coil (40% of total) at superior left abdomen • Ileum • Inferior right part of coil • Ends at appendix in lower right quadrant
Small Intestine:Modifications for absorption • Length • Increase surface area • Plicae circularis • Transverse ridges of mucosa • Increase surface area • Slow movement of chyme • Villi • Move chyme, increase contact • Contain lacteals: remove fat • Microvilli: • Increase surface area • Modifications decrease distally
SECRETION 1800 ml of intestinal juice per day Most is water that enters by osmosis across epithelial lining since chyme from stomach is very concentrated Duodenal glands also secrete mucous to protect lining Sympathetic stimulation inhibits duodenal glands…thus duodenal ulcers are stress-related Digestive enzymes come from stomach (with chyme), pancreas and liver (more later) ABSORPTION In each villus, nutrients diffuse into abundant capillaries Fats and protein/fat packages are taken up by lacteals (too big to diffuse directly into circulation Lacteals are modified lymph capillaries. Fats enter circulation by movement through lymph vessels, eventually to thoracic duct Secretion and absorption in small intestines
Large Intestines • Frame around rest of gut • Ascending, transverse, descending • Starts at cecum/appendix • Ends at rectum, anal canal • Teniae coli • “ribbons” or strips of muscle along length of colon (three around tube) • Tension in teniae coli forms haustra or sacs • Little continuous movement, but mass peristaltic movement several times daily to force feces towards rectum • Absorption of water from food
Rectum + Anal Canal • Rectum • descends into pelvis • no teniae coli • longitudinal muscle layer complete • rectal valves • Anal Canal (more with pelvis) • passes through levator ani muscle • releases mucus to lubricate feces • Internal anal sphincter • involuntary, smooth m. • External anal sphincter • voluntary, skeletal m.
Blood supply--ventral branches off of aorta • Celiac a.--to stomach, liver, pancreas, spleen, duodenum • Superior (cranial) mesenteric a.--to small intestines and most of colon • Inferior (caudal) mesenteric a.--to descending colon, rectum
Innervation of gut VAGUS • Parasympathetic • What nerve? • Where does it run? • Sympathetic • Only thoracic output from spinal cord • Splanchnic nerves from thorax lateral to vertebral bodies bring posteriorly to abdominal cavity and gut • Synapse in celiac and superior mesenteric ganglia • Both Para- and Sympathetic follow aa. out to organs • Enteric nervous system: High level of local control with network of synapses within ganglia and around gut With aorta
Digestive Hormones also control secretion and absorption • Table 24-2