Download
1 / 23
230 likes | 306 Views
Changing Patterns of NRTI and PI Resistance Mutations Between 2006 and 2011 in ART experienced SA patients. Gert van Zyl 1 , Mathilda Claassen 1 , Susan Engelbrecht, 2 Tulio De Oliveira 2 , Wolfgang Preiser 3 , Natasha Wood 4 , Simon Travers 4 , Robert Shafer 5.

E N D
Changing Patterns of NRTI and PI Resistance Mutations Between 2006 and 2011 in ART experienced SA patients Gert van Zyl1, Mathilda Claassen1, Susan Engelbrecht,2TulioDe Oliveira2, Wolfgang Preiser3, Natasha Wood4, Simon Travers4, Robert Shafer5 1National Health Laboratory Service, Tygerberg, Coastal Branch, South Africa; 2Division of Medical Virology, Stellenbosch University, Faculty of Health Sciences, Parow, South Africa; 3Africa Centre for Health and Population Studies, University of KwaZulu-Natal, South Africa; 4South African National Bioinformatics Institute(SANBI), University of Western Cape, South Africa; 5Division of Infectious Diseases, Center for AIDS Research, Stanford University Medical Center, Stanford, CA, United States of America
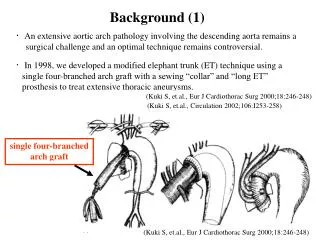
Background (1) • Toxicity of stavudine(D4T), resulted in it being replaced by TDF in adults and ABC in children, for South African patients, newly initiated on therapy since April 2010 • In addition, in patients with symptoms or signs of toxicity, TDF or ABC could substitute D4T or AZT • This resulted in a rapid increase in the use of TDF in adults and ABC in children
Background (2) • In vitro data suggests that sub-type C strains may be more prone to developing the K65R mutation • However the particular TDF drug combination used may be a stronger predictor (Tang et al. 2012) of K65R • Limited data on the prevalence of TDF associated mutations (K65R, Y115F, K70E) and ABC associated mutations (L74V/I, Y115F) in patients in SA receiving these ‘new’ regimens. • Study conducted to assess the prevalence of resistance associated mutations (RAMs) when virologic failure occurs and associations with particular regimens.
Methods(1) Study population • Specimens received from over South Africa, from many public health hospitals and clinics, majority from Gauteng and Western Cape Provinces. • Doctors complete a request form that is used for antiretroviral roll-out (designed for CD4 and VL monitoring) and contains a limited field for current therapy only.
Methods(2) Test method: • Validated in-house antiretroviral genotypic resistance assay was used: spans PR and amino acids 1-262 of RT Sequence processing: • Nucleotide FASTA files, from all patients were imported and resistance interpretations performed using Sierra, The Stanford HIV Web Service (Version 1.0). Inclusion: • Patients with sequence AND recorded current therapy were included • 1525 specimens (from 1293 patients) from May 2006 to September 2011
D4T/TDF/ABC + 3TC associated with different NRTI mutation patterns
TDF associated RAMs frequency also dependent on other regimen components A62V – restores fitness ~ K65R
Patients on NVP may be more likely to have TDF-associated mutations p=0.009
Mutations when ABC+ 3TC is used with PI or NNRTI Fewer patients on LPV/r had ABC associated RAMs; p< 0.001
LPV-associated major PI resistance mutations Patients with major PI resistance: n=42
DRV RAMs in about 4% of patients on LPV RTV as single PI historically used?
EFV and NVP select different mutations EFV vs. NVP for: V106M and Y181C p< 0.001
Conclusion (1) • When antiretroviral failure occurs on a TDF regimen a high prevalence of TDFRAMs (K65R, Y115F, K70E or A62V) are observed – this concurs with other SA data (Sunpathet al. CROI 2012) • The prevalence of TDF RAMs may be more common after NVP failure (7/8) than EFV (40/105) failure. • Failure on an ABC regimen is associated with a high prevalence of L74V/I or Y115F. • LPV/r regimen protects against TDF- or ABC- RAMs.
Conclusion (2) • Prevalence of major PI resistance mutations ~ 10% in LPV/r treated patients who fail (similar UK cohort, Barber et al. 2012) • 14 of 42 with LPVassociated RAMs have DRV cross resistance • Historic use of RTV as single PI in children could have contributed to relative high prevalence of PI resistance
Conclusion (3) • Although the prevalence of TDF-associated mutations on TDF failure is high – current data shows that the TDF, FTC/3TC, EFV failure rate is low. • D4T therapy failure results in a therapeutic dilemma – unknown whether patient has K65R or TAMs – and whether AZT or TDF should be preferred • In contrast, on TDF or ABC regimen failure, RAMs are predictable and second-line options are likely to be effective.
Acknowledgements • Specimens and results: We would like to thank Ronell Taylor, who compiled the database, the clinicians across South Africa, who provided specimens and clinical information, and National Health Laboratory Service technologists, who received the specimens and processed them. • Database support: We would like to thank Tommy Liu, Stanford Resistance Database, for support with Sierra, The Stanford HIV Web Service.