Download
1 / 50
520 likes | 681 Views
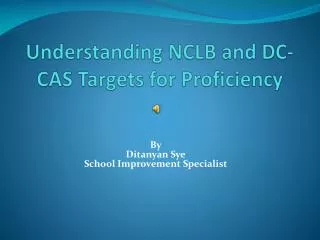
Is lower better? LDL targets and beyond. Implications of the relationship between risk factor (LDL-C) level and event rate. LOG of event rate. Event rate. Risk factor level. Risk factor level. 1: Is there a continuous relationship? 2: Is there a lower limit?

E N D
Implications of the relationship between risk factor (LDL-C) level and event rate LOG of event rate Event rate Risk factor level Risk factor level 1: Is there a continuous relationship? 2: Is there a lower limit? 3: What is the nature of the relationship? Log – linear: No lower limit Law of diminishing returns
LDL-lowering lowers the risk ofMAJOR CARDIOVASCULAR EVENTSand more lowering provides more benefit 20 Control 21% relative risk reduction in CVD per mmol/L Statin 15 More statin 16% relative risk reduction in CVD per 0.5 mmol/L Five year risk of a major vascular event, % 10 Combined evidence: 33% relative risk reduction per 1.5 mmol/L (since 0.79 x 0.84 = 0.67) 5 0 0 1 2 3 4 5 Lancet 2010 LDL cholesterol, mmol/L
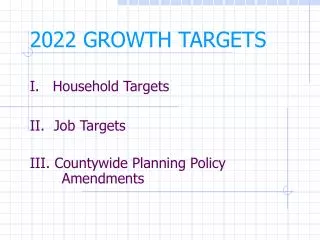
Implications of the relationship between risk factor treatment and event rate. Is there a “J” curve? Event rate Treated risk factor level: Antihypertensive & hypoglycaemic therapy in ACCORD Trial adverse What is the Harm : Benefit ratio for LDL reduction?.
Cholesterol PLA2 Cholesteryl esters FAS ECH1 CPT1 PexIIa ACAT ACAT Cholesterol apoE apoA1 Ox chol and LXR oxLDL CD36 SR TG-rich lipoproteins Lipid Uptake & Synthesis PG, LTs FFAs oxysterols LPL FAS TATA TATA PPAR/RXR RXR/LXR ABCA1 ABCG1 apoE LPL SREBP1c CD36 LXRα Cpt1 Ech1 PexIIa LPL FFAs Lipid Catabolism, Efflux & Storage Many animal species, neonates, and patients with genetic diseases tolerate very low LDL-C FAS FFAs Mitochondria β oxidation ABCA1
Theoreticallypredictedrisk Observedrisk PCSK9 R46L Non-carriers Heterozygotes Homozygotes P=0.54 Is low LDL a causative risk factor for non-CVD morbidity and mortality? ABCG8 D19H Non-carriers Heterozygotes Homozygotes P=0.78 • Cancer and chronic disease reduce LDL-C rather than vice-versa • Need to adjust for undiagnosed cases • “Mendelian randomisation” re LDL-C and cancer : not associated APOE ε2/ε3/ε4 44 43 33 42 32 22 P=0.96 Hazard/odds ratio for Cancer (95% CI)
Does LDL lowering lead to a net increase in risk (ie via non-CVD events)? • Significant decrease in CV. • Even in “low risk” • AR <5% NNT 167 • AR 5-10% NNT 67 • No increase in non-CVD • NNH diabetes 250 • NNH H’ stroke 1000 • NNH myopathy 10000 • NNH rhabdo 50000
“Reversal Trial” benefit at <1.6 mmol/l “TIMI 22” & “TNT” benefit at <2 mmol/l ATP interim target in high risk <1.8 mmol/l PBS review recommendation <2.0mmol/l “IDEAL” Simvastatin 20 mg vsAtorvastatin 80 mg LDL = 2.5 vs 2 mmol/l 11% benefit (ns) over 4.8 y The special case of Familial Hypercholesterolaemia Often sole risk factor Untreated LDL-C often >> 5 mmol/l Aim to reduce untreated LDL-C by > 50% How were lower LDL-C Targets decided?
Small LDL Cholesterol ester Triglyceride Lipase TG affects cholesterol content, and hence size, composition and density of lipoproteins TG CETP CE When TG is elevated LDL-C may under-estimate LDL particle number and CVD risk. Otvos JD, et al. AJC 2002;90(8A):22i-29i
CVD risk is proportional to the number of atherogenic lipoproteins rather than their cholesterol content (or composition). • Quebec Cardiovascular Study • Apo B: 1 per particle LDL particle number (Apo B) Risk of IHD LDL particle size Lamarche B, et al. Circulation 1997; 95:69-75
Is LDL – C the best target? US Health Professionals Study • Quintile 5 vs. Quintile 1 • P-Trend is a test for a rise or fall in RR from Q1 to Q5 Pischon et al. Circulation 2005;112:3375-3383.
Measured LDL-C 2.5 mmol/l Measured LDL-C 2.5 mmol/l LDL particles 1600 nmol/L LDL particles 900 nmol/L NMR Measures LDL Particle NumberNot LDL Cholesterol VLDL LDL NMR Signals LDL
Outcome Associations of NMR LDL Particle Number (LDL-P) versus LDL Cholesterol (LDL-C) * Significant and independent after multivariate modeling (lipids and established risk factors)
Effect of LDL Lowering Therapies on LDL-C, Non-HDL-C, Apo B, and LDL-P Sniderman AD. J Clin Lipidology 2008;2:36-42
LDL-C may underestimate reduction in LDL particle number: • Fibrates • Niacin • Pioglitazone • Omega 3 FAs • Exercise • Mediterranean and • low carb diet • LDL-C may overestimate reduction in LDL particle number: • Statins • Statin + Ezetimibe or Bile • Acid Sequestrants • Estrogen Replacement • Therapy • Anti-retrovirals (some) • Low fat, High carb diet Therapy LDL-P More Than LDL-C Therapy LDL-C More Than LDL-P Treatments That Alter Cholesterol Content of LDL Change LDL-C and LDL-P Differentially • Little Change in Cholesterol per Particle with: • Bile Acid Sequestrant or EzetimibeMonotherapy Similar Change in LDL-C and LDL-P Cromwell WC. In: Clinical Challenges in Lipid Disorders.Toth PP, Sica DA, editors. Oxford: Clinical Publishing; 2008.p. 249-259.
Current treatment LDL-C lowering treatment options Maximum tolerated statin dose Maximum statin + Ezetimibe Maximum statin + Ezetimibe + Niacin &/or BAS resin Maximum statin + Ezetimibe + Niacin + BAS resin Depending on NHDL-C, apo B etc, consider fibrates & n-3 If desperate, consider plasmapheresis New treatment options currently under investigation
Future LDL-C treatment options • Antibodies or antisense oligonucleotides against PCSK9 • Highly potent CETP Inhibitors can reduce LDL-C and Lp(a) • Anacetrapib and Evacetrapib • LXR inhibitors cause fatty liver: Target related mechanisims • IDOL (Inducible degrader of LDL Receptor)? • Trans intestinal cholesterol transport • Inhibitors of atherogenic lipoproteins also cause fatty liver • Judicious use of Apo B antisense oligonucleotide (Mipomersin) • Judicious use of Microsomal Transfer Protein (MTP) inhibitors • Less likely: Eprotirome, Inhibitors of SqualeneSynthase or ACAT
Blockade of PCSK9/LDLR Interaction May Lower LDL Levels 1. Chan JC, et al. Proc Natl Acad Sci U S A. 2009;106:9820-9825.
Cellular sterol regulation: LXR reduces LDL-R uptake via IDOL (Inducible degrader of LDL-receptor) LDLR LDLR ABCG1 ABCA1 LXRs IDOL cholesterol uptake cholesterol biosynthesis + + + HMGCoAR cholesterol efflux - ubiquitin - SREBP Statins (oxysterol, GW, T) high intracellular sterol level Zelcer et al. Science 2009;325:100-104 low intracellular sterol level
LXR promotes LDL excretion by direct Trans Intestinal Cholesterol Excretion
Options for further LDL-C reduction: Mipomersin and MTP inhibitors Hepatocyte or Enterocyte Endoplasmic Reticulum Degradation mRNA MTP = Microsomal TG Transfer Protein Membrane Ribosome VLDL Precursor + MTP/Lipid Cytosol Nascent apoB interacts with lipid free MTP and is ubiquinated apoB Golgi Endosomal free & esterified cholesterol apoB associates with MTP-Lipid complexes and forms a VLDL precursor which after lipidation with TG becomes a mature VLDL in the Golgi Mature VLDL or Chylomicron Triglycerides
LDL-C reduction: A treatment of last resort? • Prevention of unexplained or resistant CVD risk: • Attributable to unknown or novel risk factors: Lp(a), Ch 9p22 etc • Progression despite optimal treatment of other classic modifiable risk factors (such as BP, Glucose etc) to the lower end of physiological range • Due to “hard to treat” risk factors such as isolated low HDL-C • LDL-C lowering therapy to achieve levels well below the usual physiological range appears to be safe and effective
Mrs E. T. Mrs E.T is a slightly overweight (BMI 26) woman with type 2 diabetes, which was diagnosed 11 years ago. She is normotensive on Atacand 16 mg, ACR is within normal limits but eGFR is 55mls/min. HbA1C is 6.9%. ECG suggested silent AMI, so Atorvastatin was increased to 40 mg.nocte. Follow-up lipids include: TC=3.9, TG=2.5, HDL=1.1, LDL=1.7 mmol/l.
Questions concerning Mrs E.T. LDL-C and HDL-C are within target levels. Are you satisfied with lipid control? Yes/No Which of the following would assist your assessment? A) TC/HDL ratio B) TG/HDL ratio C) Apo A1 D) Apo B E) Apo A1:ApoB ratio A renal dose (48mg) of fenofibrate is commenced. Would you be discouraged if LDL-C increased? Yes/No Mrs E.T. Is concerned about the increase in statin does and the prospects of low cholesterol because of media reports that breast cancer rates were increased in the CARE trial. You can reassure her that this finding has been refuted. True / False
Mrs E.T is a slightly overweight (BMI 26) woman with type 2 diabetes, which was diagnosed 11 years ago. She is normotensive on Atacand 16 mg, ACR is within normal limits but eGFR is 55mls/min. HbA1C is 6.9%. ECG suggested silent AMI, so Atorvastatin was increased to 40 mg.nocte. Follow-up lipids include: TC=3.9, TG=2.5, HDL=1.1, LDL=1.7 mmol/l. LDL-C and HDL-C are within target levels. Are you satisfied with lipid control? Yes/No Which of the following would assist your assessment? A) TC/HDL ratio B) TG/HDL ratio C) Apo A1 D) Apo B E) Apo A1:ApoB ratio Mrs E.T. Is concerned about the increase in statin does and the prospects of low cholesterol because of media reports that breast cancer rates were increased in the CARE trial. You can reassure her that this finding has been refuted. True / False
LDL-C and HDL-C are within target levels. Are you satisfied with lipid control? Yes No
“AtheroDyslip” • ↑TG/VLDL-C • SD LDL • ↓HDL-C Kidney TG LDL Rapid Degradation Apo A-I SDLDL Hepatic Lipase HDL SD HDL HDL SDLDL LDL-C and HDL-C are within target levels. Are you satisfied with lipid control?The case for “no” 1 Liver VLDL-C CE FFA/TG CETP VLDL ↑Central Adiposity TG 3 CE CETP TG 2 Insulin Resistance Hepatic Lipase CETP = cholesterol ester transfer protein
Which of the following would assist your assessment? A) TC/HDL ratio B) TG/HDL ratio C) Apo A1 D) Apo B E) Apo A1:ApoB ratio
Which of the following would assist your assessment?The case for “D”
A renal dose (48mg) of fenofibrate is commenced. Would you be discouraged if LDL-C and creatinine increased? Yes No
A renal dose (48mg) of fenofibrate is commenced. Would you be discouraged if LDL-C and creatinine increased?The case for “No” 16 14 12 5-year CVD Event Rate (%) 10 8 6 4 2 0 Placebo Placebo Fenofibrate creatinine <78 78-94 >94 <78 78-94 >94
You can reassure her that this finding (increased breast cancer) has been refuted.... True False
You can reassure her that this finding (increased breast cancer) has been refuted....The case for “true” Ahern TP, Pedersen L, Tarp M et al. Statin Prescriptions and Breast Cancer Recurrence Risk: A Danish Nationwide Prospective Cohort Study. Journal of the National Cancer Institute (2011) 103 : 1461-1468. RESULTS: Most prescriptions for lipophilicstatins in the study population were for simvastatin. Exclusive simvastatin users experienced approximately 10 fewer breast cancer recurrences per 100 women after 10 years of follow-up (adjusted 10-year risk difference = -0.10, 95% confidence interval = -0.11 to -0.08), compared with women who were not prescribed a statin. Exclusive hydrophilic statin users had approximately the same risk of breast cancer recurrence as women not prescribed a statin over follow-up (adjusted 10-year risk difference = 0.05, 95% confidence interval = -0.01 to 0.11).
More questions concerninig Mrs E. T. Despite this, Mrs E.T. subsequently suffers an acute coronary syndrome and aspirin has been commenced. Would you A) Intensify antihypertensives although BP is 118/75 B) Intensify oral hypoglycaemics although HbAIC is < 7% C) Intensify fibrate although TG and HDL are now at target (<2mmol/l and > 1 mmol/l respectively) D) Intensify LDL-lowering although LDL-C is < 1.8 mmol/l E) Rely on the addition of aspirin to avoid further events? You add ezetimibe and LDL-C falls to < 1.0 mmol/l. Is this safe? Yes / No Mrs E.T. Starts a trial of addition of a CETP inhibitor. You are not blinded to her lipid results, which include: TC = 3.2, TG=1.7, HDL=2.4 mmol/l, so you calculate LDL-C as zero. Should you believe this result? Yes / No
Despite this, Mrs E.T. subsequently suffers an acute coronary syndrome and aspirin has been commenced. Would you.... Intensify antihypertensives although BP is 118/75 B) Intensify oral hypoglycaemics although HbAIC is < 7% C) Intensify fibrate although TG and HDL are now at target (<2mmol/l and > 1 mmol/l respectively) D) Intensify LDL-lowering although LDL-C is < 1.8 mmol/l E) Rely on the addition of aspirin to avoid further events?
You add ezetimibe and LDL-C falls to < 1.0 mmol/l. Is this safe? Yes No
You add ezetimibe and LDL-C falls to < 1.0 mmol/l. Is this safe?The case for “Yes” Ann Surg. 2010 Jun;251:1034-40. Overall mortality, incremental life expectancy, and cause of death at 25 years in the program on the surgical control of the hyperlipidemias. Buchwald H, Rudser KD, Williams SE, Michalek VN, Vagasky J, Connett JE. There were 838 patients randomized in POSCH (421 surgery, 417 control). At 25 years follow-up, the difference was statistically significant, with survival probabilities of 0.57 (surgery) and 0.51 (controls). Cause of death data indicated a significant increase in cardiovascular deaths in the control group; cancer deaths were also greater in the control group but this was not significant. The estimated incremental increase in life expectancy over more than 25 years of follow-up was 1.0 year overall and 1.7 years in the cohort with an ejection fraction > or = 50%.
Mrs E.T. starts a trial of addition of a CETP inhibitor. You are not blinded to her lipid results, which include: TC = 3.2, TG=1.7, HDL=2.4 mmol/l, so you calculate LDL-C as zero. Should you believe this result? Yes No
sdLDL LIPASE TG TG CETP CETP CE CE Mrs E.T. starts a trial of addition of a CETP inhibitor. You are not blinded to her lipid results, which include: TC = 3.2, TG=1.7, HDL=2.4 mmol/l, so you calculate LDL-C as zero. Should you believe this result?An explanation of “No” VLDL HDL LDL FATTY ACIDSGLYCEROL Inhibition of CETP will invalidate the assumptions about VLDL composition that form the founndation of the Friedewald equation LDL-C = Total-C – HDL-C – (TG/2.2) mmol/l
Ms J.A. Mrs J.A. Is a 27 year old woman who has recessively inherited Microsomal Transfer Protein (MTP) deficiency that prevents her from lipidatingapo B-containing lipoproteins. Her lipid profile features: TC=2.7, TG=0.4, HDL=2.3, LDL = 0.2 mmol/l
Questions concerning Ms J.A. Which organ systems are likely to be adversely affected in this condition (more than 1 answer is possible) A) Cardiovascular B) Neurological C) Renal D) Gastrointestinal E) Respiratory Diet should include: A) More fat B) Less fat C) Extra Fat Soluble Vitamins D) A + C E) B + C Ms J.A plans to start a family: Is her reproductive capacity diminished by the very low levels of LDL-C? Yes /No Treatment up until now has avoided any consequences. Is Ms J.A.’s life expectancy A) Decreased B) Unaltered C) Increased
Which organ systems are likely to be adversely affected in this condition (more than 1 answer is possible) A) Cardiovascular B) Neurological C) Renal D) Gastrointestinal E) Respiratory
Which organ systems are likely to be adversely affected in this condition?The case for “B” and “D” Malabsorption syndrome Erythrocyte sedimentation rate low Anemia Acanthocytosis Hepatic steatosis Nystagmus Short stature Retinitis pigmentosa Demyelination Diarrhoea Kyphosis Cerebellar syndrome
Diet should include: A) More fat B) Less fat C) Extra Fat Soluble Vitamins D) A + C E) B + C
Diet should include:The case for “E” DEFICIENCY OF FAT SOLUBLE VITAMINS Nystagmus Retinitis pigmentosa Demyelination Cerebellar syndrome KyphosisShort stature INABILITY TO TRANSPORT FAT Malabsorption syndrome Hepatic steatosis Diarrhoea
Ms J.A plans to start a family: Is her reproductive capacity diminished by the very low levels of LDL-C? Yes No
Questions concerning Ms J.A. Ms J.A plans to start a family: Is her reproductive capacity diminished by the very low levels of LDL-C?The case for “No”
Treatment up until now has avoided any consequences. Is Ms J.A.’s life expectancy A) Decreased B) Unaltered C) Increased
Treatment up until now has avoided any consequences. Is Ms J.A.’s life expectancyThe case for “increased” Familial HypobetalipoproteinemiaAbsence of Atherosclerosis in a Postmortem Study Jeffrey A. Kahn, MD; Charles J. Glueck, MD JAMA. 1978;240:47-48. Men and women from hypobetalipoproteinemickindreds had reported life expectancies that were seven and six years longer, respectively, than for US white populations (P<.002).2 Combined myocardial infarction morbidity and mortality was 2.5% in hypobetalipoproteinemickindreds, fivefold less than in normolipemic controls (11%; P<.01).2 In hypobetalipoproteinemia, low C-LDL, the atherogenic lipoprotein,2-4 or a low ratio of C-LDL to C-HDL, the antiatherogenic lipoprotein,2,4 may facilitate longevity and decrease morbidity and mortality from myocardial infarction.2