Download
1 / 40
480 likes | 1.07k Views
LENS. It is a highly organized transparent spheroid structure that has evolved to perform refraction of the light entering in the eye. It does not posses nerve, blood vessels or connective tissue. . Anatomy of LENS. Biconvex Lens Diameter varies from 8.8 to 9.2 (9mm)

E N D
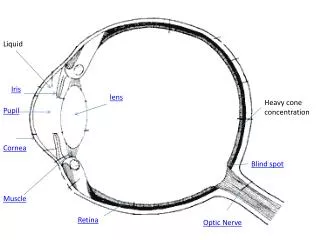
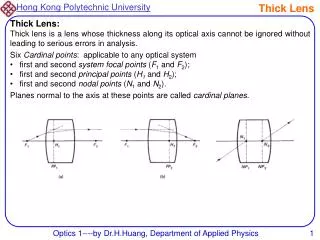
LENS It is a highly organized transparent spheroid structure that has evolved to perform refraction of the light entering in the eye. It does not posses nerve, blood vessels or connective tissue.
Anatomy of LENS • Biconvex Lens • Diameter varies from 8.8 to 9.2 (9mm) • Lens grow in size continuously throughout life. Its weight is about 60 mgm at the birth and up-to 250 mgm by 80 years of age. • Antero-posterior thickness changes with accommodation. Thickness is 4.75 – 5 mm (4.5mm) (un-accommodated) in adults. • Circumference is known as equator
Anatomy of LENS • Lens is suspended in eye by Zonules which are inserted on anterior surface and equatorial lens capsule and attached to ciliary body(Pars Plicata- Ciliary Processes) . • Zonular fibres are series of fibrillin rich fibre.
Anatomy of LENS Histologically lens consists of three major components: • 1. Capsule – is a thick collagenese basement membrane which is transparent, elastic acellular envelop, thick at anterior pre-equatorial region (21 micron m), thinnest at the posterior pole (4 micron m). Anterior pole is approximately 14 micron m thick.
Anatomy of LENS • 2. Lens Epithelium – It is a single layer of cells lining the anterior capsule and extends to the equatorial lens bow. Zone of epithelial cells: a. Central – cells do not actively divide, they divide under pathological conditions only. b. Pre-equatorial germinal zone : cells rarely divide.
Anatomy of LENS C. Germinal zone: constitute of the stem cell population. The newly formed cells from germinal zone are forced into transitional zone where they elongate and differentiate to form mass of the lens. The lens capsule regulate the transport of metabolite, nutrients and electrolytes to the lens fibers.
Anatomy of LENS • 3. Lens substance: It constitute the main mass of the lens. It is divided into- a. Nucleus b. Cortex Nucleus: consists of (i) Embryonic nucleus (it contains primary lens fibres that are formed in lens vesicle)
Anatomy of LENS (ii) Fetal nucleus: it contains embryonic nucleus and all fibres added to the lens before birth (iii) Infantile nucleus: it contains embryonic , fetal nucleus together with all the fibres added up-to the age of 4 years. (iv) Adult nucleus: composed of all fibres added before sexual maturation The nucleus consists of densely compacted lens fibres and higher refractive index than cortex.
LENS Anatomy Cortex Capsule 3 4 5 3 – Adult Nu 4 - Infantile Nu 6 5 – Foetal Nu 6 – Embryonic Nu.
Lens Cortex It is located peripherally and is composed of secondary fibres formed continuously after sexual maturation. It is further divided into: • Deep cortex • Intermediate cortex • Superficial cortex
LENS- Crystalline Lens fibres contain high concentrations of crystalline. Crystalline represent the major protein of the lens (constitute 90% of total protein content of lens). Crystalline has the following constituents: Alpha Beta and, Gamma
Lens - Functions The lens serves two major functions: • Focusing of visible light rays on the fovea • Preventing damage from ultra-violet radiation by reaching the retina
Lens – Physiology • Lens function and transparency is dependant on the supply of appropriate nutrient to its various structures. Metabolic needs of a adult lens is met by the aqueous and vitreous. • There is continuous transport of ions into and out of the lens.
Lens – Physiology • The transparency is dependent on highly organized structure of lens, dense packing of crystalline. Avascularity, absence of pigments and optimal hydration. • By act of accommodation it changes focusing power. Accommodation occurs by increasing the curvature of anterior surface thereby changing refractive power of lens. • Light transmission and elasticity of lens decreases with age.
CATARACT • Any opacity in the lens or its capsule, whether developmental or acquired is called cataract. • Developmental opacities are usually partial and stationary, whereas acquired opacities are progressive. They progress until the entire lens is involved, but exceptions are well known in both types.
Classification of Cataract • Classification based on Etiology • Classification based on Morphology • Classification based on Maturity • Classification based on the Age of onset
Classification based on Etiology • Developmental • Acquired
Developmental • Hereditary • Intrauterine causes • Rubella • Toxoplasmosis • CMV • Steroids
Acquired Cataract • Age related (senile) • Secondary cataract (Chronic Uveitis, ACG) • Cataract associated with ocular diseases • Cataract associated with systemic diseases (pre-senile) (Diabetes, galactosemia etc) • Traumatic Cataract • Drug induced cataract (Steroids and others)
Classification based on Morphology • Capsular (Ant and Post) • Subcapsular (Ant and Post) • Nuclear • Cortical
Classification based on Maturity • Immature • Mature • Hypermature • Morgagnian
Classification based on the Age of onset • Congenital • Infantile • Juvenile • Presenile • Senile
Risk Factors for Cataract • Senility • Sunlight (specially UV –A and UV-B component) • Severe Diarrheal dehydration • Vitamin A,C, E deficiency • Diabetes • Smoking • Corticosteroids • Genetic
Pathogenesis of Cataract • Caused by degeneration and opacification of existing lens fibres, formation of aberrant fibres or deposition of other material in their place. • Factors causing disturbance of critical intra – and extra-cellular equilibrium of water and electrolyte or deranges the colloid system within the fibres tends to bring about opacification.
Pathogenesis of Cataract • Fibrous metaplasia of fibres (in complicated cataract) • Epithelial cell necrosis (Glaucomflecken) • Deposition of abnormal products of metabolism, drugs or metals.
Pathogenesis of Cataract • Biochemical Processes • Hydration • Denaturation of Lens Proteins • Sclerosis
Pathogenesis of Cataract • The Changes in the Epithelial Cells and the Capsule • Changes in the Lenticular Fibres • Sclerosis
Symptoms of Cataract 1. Blurring of vision 2. Frequent change of glasses due to rapid change in refractive index of the lens 3. Painless, progressive gradual diminution of vision due to reduction in transparency of the lens 4. Second sight or myopic shift in case of nuclear cataract causing index myopia, improving near vision.
Symptoms of Cataract 5. Loss or marked diminution of vision in bright sunlight or bright light beam in central posterior subcapsular cataract. 6. Monocular diplopia or polyopia in presence of cortical spoke opacities 7. Glare in posterior subcapsular cortical cataract due to increased scattering of light
Symptoms of Cataract 8. Colored haloes around the light as seen in cortical cataract due to irregular refractive index in different parts of the lens. 9. Color shift , reds are accentuated 10. Visual field loss, generalized reduction in sensitivity due to loss of transparency
Disturbances in Vision • Appearance of Black Spots • Reduction of Visual Fields • Uni ocular Polyopia • Lenticular Myopia • Changes in Colour values
Differential Diagnosis of painless gradual diminution of vision • Chronic open angle glaucoma • Macular degeneration • Optic atrophy • Corneal dystrophy • Retinopathy associated with systemic disorders (hypertension or diabetes)
Assessment • Visual Acuity • Direct Distant Ophthalmoscopy (Fundal Glow) • Light Reflex • Slit Lamp Examination
Management • Medical • Surgical
Medical Management • Refraction • Dark Glasses
Surgical Management Indications • Visual Improvement • Medical Indications • Cosmetic Indications
Surgical Management • Couching • Intracapsular Cataract Extraction (ICCE) • Extracapsular Cataract Extraction (ECCE) • Phacoemulsification
Clinical Rotation of 3rd Year • Surgical Techniques • Complications • Management of complications
EctopiaLentis • Aquired(Trauma, Large eye ball, High Myopia) • Hereditary • Marfans Syndrome • Homocystinuria • Weil Marchesani Syndrome