Download
1 / 52
520 likes | 666 Views
The Medicare Appeals Process. Navigating the Medicare Maze. Chiropractic Services Medicare Basics.

E N D
The Medicare Appeals Process Navigating the Medicare Maze www.mybreakthrough.com
Chiropractic Services Medicare Basics • “Chiropractic service which is eligible for reimbursement, is specifically limited by Medicare to the treatment by means of manual manipulation (i.e., by use of the hands or use of manual devices that are hand-held, with the thrust of the force of the device being controlled manually) of the spine for the purpose of correcting a subluxation.” www.mybreakthrough.com
The Medicare Carriers Manual • The Medicare Carriers Manual (the Manual) outlines additional coverage criteria for chiropractic services billed to Medicare. • Pursuant to section 2251.2 of the Manual, the existence of a subluxation must be documented through an x-ray or physical examination and chiropractic services must be provided as part of a written plan of care that should include specific goals and measures to evaluate effectiveness. • Section 2251.3 of the Manual states that chiropractic treatment “. . . Must provide a reasonable expectation of recovery or improvement of function.” www.mybreakthrough.com
CMS Subluxation Definition • “For Medicare purposes, subluxation is defined as a motion segment in which alignment, movement integrity and/or physiological function of the spine are altered although contact between joint surfaces remains intact.” www.mybreakthrough.com
Chiropractic Services CMS Basics • CPT Codes paid by CMS to Chiropractors… • 98940 (Chiropractic Manipulation, 1-2 Regions) • 98941 (Chiropractic Manipulation, 3-4 Regions) • 98942 (Chiropractic Manipulation, 5 Regions) • CPT codes not paid by CMS to Chiropractors… • 98943 (Chiropractic Manipulation / Extraspinal) • All Exams, Therapies, X-rays, DME, Etc. www.mybreakthrough.com
Medicare Reimbursement www.mybreakthrough.com
Do You Know Your Carrier? • What can you do on your carrier’s website? • Look up fee schedules • Review policy and procedure • Find your Local Coverage Determinations (LCDS) • Sign up for bulletin board notices • Get training • Use the Interactive Voice Response (IVR) System www.mybreakthrough.com
Medicare Administrative Contractors (MAC) Jurisdictions • CMS uses a network of contractors called Medicare Administrative Contractors to process Medicare claims, enroll health care providers in the Medicare program and educate providers on Medicare billing requirements. • MACs also handle claims appeals and answer beneficiary and provider inquiries. www.mybreakthrough.com
Consolidated Medicare A/B MAC Jurisdictions www.mybreakthrough.com
Who Is Eligible for Medicare? • Seniors who are 65 or over; paid the Federal Insurance Contributions Act (FICA) tax minimums • Disabled or qualified through state SSI • End-Stage Renal Disease www.mybreakthrough.com
Medicare Parts • Medicare Part A: Hospital, CORF, Skilled Nursing • Medicare Part B: Physician based services • Medicare Part C: Medicare Advantage /Managed Care • Medicare Part D: Prescription Drug Plans www.mybreakthrough.com
Medicare Participation www.mybreakthrough.com
To Participate or Not to Participate? • Yearly opt-in/opt out of participation • Different than “Accepting Assignment” • Different than opting in/out of Medicare www.mybreakthrough.com
Can DCs Opt Out of Medicare? • The short answer is, no. • DCs may not “opt out” or privately contract with Medicare patients for the delivery of services outside of Medicare fee limitations and filing requirements. • According to the Medicare Benefit Policy Manual (Chapter 15, Section 40.4), “the opt out law does not define ‘physician’ to include chiropractors; therefore, they may not opt out of Medicare and provide services under private contract.” www.mybreakthrough.com
“Par” versus “Non-par” • The primary difference between the two statuses lies in how you collect your fees. • Participating providers must accept assignment (wait for payment directly from Medicare), while non-participating providers may collect up-front from the patient (non-assigned claims). www.mybreakthrough.com
Patient ResponsibilityParticipating Providers • Provider bills regular fee if they want • Medicare will pay 80% of par-allowance • Patient responsible for 20% of par-allowance • Secondary will pay 20% of par allowance • If secondary allows, may pay other charges as well www.mybreakthrough.com
Patient ResponsibilityNon Par Providers • Providers charge the limiting charge, 115% of non-par allowance • Reimbursed at 95% of par allowance • You are still bound by all the other rules if non-par • You can accept assignment case-by-case • Reimbursement is still non-par allowance www.mybreakthrough.com
Changing Your Status • Typically providers are given the last six weeks of the calendar year (Nov. 15-Dec. 31) to change their participation status. • Once made, the decision is binding throughout the following calendar year (unless the decision period is re-opened). • Another exception could be in situations where a physician’s practice changes significantly, such as relocation to a different geographic area or transformation into a group practice. www.mybreakthrough.com
Confirming Medicare Coverage • 1st make sure that patient has traditional Medicare Red / White / Blue card • Medicare Replacement Plan (Advantage—like an HMO/PPO) • Verify Secondary or Medi-Gap Coverage • Use the carrier’s IVR www.mybreakthrough.com
What is a Medicare Advantage Plan? • A Medicare Advantage Plan (like an HMO or PPO) is another Medicare health plan choice qualified beneficiaries may have as part of Medicare. • Medicare Advantage Plans, sometimes called “Part C” or “MA Plans,” are offered by private companies approved by Medicare. • If your patient joins a Medicare Advantage Plan, the plan will provide all Part A (Hospital Insurance) and Part B (Medical Insurance) coverage. • Medicare Advantage Plans may offer extra coverage, such as vision, hearing, dental, and/or health and wellness programs. • Most include Medicare prescription drug coverage (Part D). www.mybreakthrough.com
What is a Medicare Advantage Plan? • Medicare pays a fixed amount for your patient’s care every month to the companies offering Medicare Advantage Plans. • These companies must follow rules set by Medicare. However, each Medicare Advantage Plan can charge different out-of-pocket costs and have different rules for how these patients get services (like whether a referral is needed to see a specialist, like chiropractors, or if they have to go to only doctors, facilities, or suppliers that belong to the plan for non-emergency or non-urgent care). • These rules can change each year. www.mybreakthrough.com
What You Must Know about Medicare Advantage • ABN forms do not apply to most Medicare Advantage plans. • Verify the insurance benefits just like you would for regular health insurance. While making that call, you would ask for both in and out of network benefits, and confirm which your office is subject to. • Should you need to appeal denials, realize that the appeals process is different from traditional Medicare. Each plan has its own appeals process that you must be aware of. • The AT modifier will usually NOT apply in this environment. Check with each plan to be sure. • Plans can choose to eliminate DCs as they only need to provide the service, and can designate a DO or MD to do so. • Don’t assume there is chiropractic coverage automatically. www.mybreakthrough.com
Correct Case Management www.mybreakthrough.com
Should This Whole Case Be Paid By Medicare? PATIENT IMPROVEMENT COURSE OF TREATMENT www.mybreakthrough.com
Should This Whole Case Be Paid By Medicare? PRACTICES TEND TO BILL AS ONE ENTIRE CASE TO CARRIERS PATIENT IMPROVEMENT COURSE OF TREATMENT www.mybreakthrough.com
Should This Whole Case Be Paid By Medicare? Active care Active care Maintenance Care Maintenance Care PATIENT IMPROVEMENT COURSE OF TREATMENT www.mybreakthrough.com
Should This Whole Case Be Paid By Medicare? Active care Active care Maintenance Care Maintenance Care GA Mod GA Mod PATIENT IMPROVEMENT New DX/ AT Mod New DX/ AT Mod COURSE OF TREATMENT www.mybreakthrough.com
Episodic Care History Taken Activities of Daily Living Discharge Summary Diagnosis Reflects Exam Functional Daily Notes Re-Exam Update DX/Plan Treatment Plan Functional Daily Notes www.mybreakthrough.com
Acute Treatment • CMS defines Acute as: A patient's condition is considered acute when the patient is being treated for a new injury, identified by x-ray or physical exam. • The result of chiropractic manipulation is expected to be an improvement in, or arrest of progression of, the patient's condition. www.mybreakthrough.com
Chronic Treatment • CMS defines Chronic as: • A patient's condition is considered chronic when it is not expected to significantly improve or be resolved with further treatment (as is the case with an acute condition), but where the continued therapy can be expected to result in some functional improvement. • Once the clinical status has remained stable for a given condition, without expectation of additional objective clinical improvements, further manipulative treatment is considered maintenance therapy and is not covered. www.mybreakthrough.com
Maintenance Therapy • CMS defines Maintenance Therapy as: • Chiropractic maintenance therapy is not considered to be medically reasonable or necessary under the Medicare program, and is therefore not payable. • Maintenance therapy is defined as a treatment plan that seeks to prevent disease, promote health, and prolong and enhance the quality of life; or therapy that is performed to maintain or prevent deterioration of a chronic condition. • When further clinical improvement cannot reasonably be expected from continuous ongoing care, and the chiropractic treatment becomes supportive rather than corrective in nature, the treatment is then considered maintenance therapy. www.mybreakthrough.com
Advance Beneficiary Notice (ABN) • This is one of the most misused forms in all of health care. • Breakthrough Coaching Form 128 is the most recent ABN. • The primary purpose for an ABN is to notify the patient that a covered service (i.e. chiropractic manipulative treatment code) for this particular visit may not be covered by Medicare. • You do not need an ABN for non-covered services.
Don’t get them signed every visit! • Some doctors believe they should get an ABN form signed every visit, “just in case”. • Per CMS, this is strictly forbidden, and would nullify all ABNs signed on this patient for your office. • You should only have this form signed by the patient when you believe beyond a reasonable doubt that this visit would be denied as not medically necessary.
When do I have one signed? • If your carrier has a published screen, such as 24 visits, then you would have an ABN signed for each visit beyond 24. • If you can’t verify whether a patient has had covered services that calendar year from another DC, have an ABN signed. • If you believe that the visit would not meet the Medicare guidelines for covered services, have an ABN signed.
Use Specific Language • The ABN must include the reason you believe the visit would not be covered. • There must be an original signature for each and every visit you believe would not be covered. • You must include the amount of the service (CMT) that you believe is not covered. • Be sure you include the GA modifier when you submit a CMT code for a service you have an ABN signed.
Denied Claims The Appeals Process www.mybreakthrough.com
Medicare Appeals • Most Insurance Processors simply give up on denied claims from Medicare. • The Appeals Process may seem labor intensive until you learn the system, but you will find that it eases with time and practice. www.mybreakthrough.com
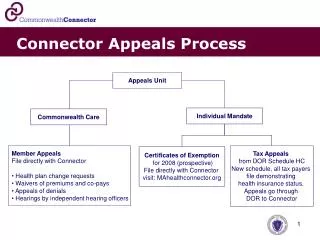
Five Levels of Appeal • Redetermination by a CMS contractor (carrier, fiscal intermediary or Medicare Administrative Contractor (MAC)) • Reconsideration by a Qualified Independent Contractor (QIC) • Hearings before an Administrative Law Judge (ALJ) within the Office of Medicare Hearings and Appeals in the Department of Health and Human Services • Review by the Appeals Council within the Departmental Appeals Board in the Department of Health and Human Services • Judicial review in federal district court www.mybreakthrough.com
Step 1: Redetermination • Performed by the contractor staff not involved in making the initial claim determination. • 120 days from initial date of denial on the EOB. • The initial determination is the Medicare Summary Notice (MSN) issued to beneficiaries, and the remittance advice (RA) issued to providers and suppliers. • The MSN and RA also include information about how to file a request for redetermination. • A minimum monetary threshold is not required to request a redetermination. www.mybreakthrough.com
Requesting a Redetermination • Follow the directions on the RA or MSN to request a redetermination. • A request for a redetermination may be filed on Form CMS-20027. • A written request not made on Form CMS-20027 must include: • Beneficiary name • Medicare Health Insurance Claim (HIC) number • Specific service and/or item(s) for which a redetermination is being requested • Specific date(s) of service • Name and signature of the party or the representative of the party www.mybreakthrough.com
Requesting a Redetermination • Attach any supporting documentation to your redetermination request. • Contractors will generally issue a decision (either a letter, MSN or RA) within 60 days of receipt of the redetermination request. www.mybreakthrough.com
Minor Errors or Omissions • Medicare enables you to correct minor errors and omissions on Medicare claims without having to go through the appeals process. • The request must be made within one year from the date of the notice of the initial determination. • You have a four-year timeframe to initiate a reopening after the date of the initial determination if good cause exists. www.mybreakthrough.com
Step 2: Reconsideration • You may request a reconsideration if dissatisfied with the redetermination. • A Qualified Independent Contractor (QIC) will conduct the reconsideration. • The QIC reconsideration process allows for an independent review of an initial determination, including the redetermination, which may include review of medical necessity issues by a panel of physicians or other health care professionals. • A minimum monetary threshold is not required to request a reconsideration. www.mybreakthrough.com
Requesting a Reconsideration • A written reconsideration request must be filed with the QIC within 180 days of receipt of the redetermination. • Check with your carrier to learn who your QIC is. • A request for a reconsideration may be made on Form CMS-20033. • If the form is not used, the written request must contain all of the following information: • Beneficiary name • Medicare Health Insurance Claim (HIC) number • Specific service(s) and/or item(s) for which the reconsideration is requested • Specific date(s) of service • Name and signature of the party or the authorized or appointed representative of the party submitting the appeal • Name of the contractor that made the redetermination www.mybreakthrough.com
Reconsideration DecisionNotification • In the request for reconsideration, you should clearly explain the reason for disputing the redetermination decision. • A copy of the RA or MRN, and any other useful documentation, should be sent with the reconsideration request. • Reconsiderations are conducted “on the record” and, in most cases, the QIC will send its decision within 60 days of receipt of the request for reconsideration. • The decision will contain information regarding further appeal rights. • If the QIC cannot complete its decision in the applicable timeframe, it will inform the appellant of their right to escalate the case to an ALJ. www.mybreakthrough.com
The Good News • Up to 60% of resubmit claims are paid at the Reconsideration stage! • Once you have passed this stage several times, very often a carrier will flag your files indicating that you have good documentation. • When you don't appeal you are only hurting yourself. • Number one: you are not getting paid! • Number two: you are letting the carrier assume that your documentation is not good enough to appeal! www.mybreakthrough.com
Individual Carrier Challenges • When you have a challenge with your individual carrier, the next level of appeal is to call your Medicare Regional Office. • There are Medicare Regional Offices located throughout the country. • Check CMS website to locate the regional office that covers your state. • The Regional Office has total jurisdiction over your carrier as a contractor and the carrier jumps when they talk! www.mybreakthrough.com
Step 3: AdministrativeLaw Judge (ALJ) • If at least $140 remains in controversy following the QIC’s decision, you may request an ALJ hearing within 60 days of receipt of the reconsideration decision. • ALJ hearings are generally held by video teleconference (VTC) or by telephone. • The ALJ will generally issue a decision within 90 days of receipt of the hearing request. www.mybreakthrough.com
Step 4: Appeals Council • If you are dissatisfied with the ALJ’s decision, you may request a review by the Appeals Council. • A minimum monetary threshold is not required. • The review must be submitted in writing within 60 days of receipt of the ALJ’s decision. • You must specify the issues and findings that are being contested. • In general, the Appeals Council will issue a decision within 90 days of receipt of a request for review. www.mybreakthrough.com
Step 5: Federal Court (Judicial) Review • If at least $1,400 or more is still in controversy following the Appeals Council’s decision, a party to the decision may request judicial review in federal district court. • You must file the request for review within 60 days of receipt of the Appeals Council’s decision. www.mybreakthrough.com