Download
1 / 1

E N D
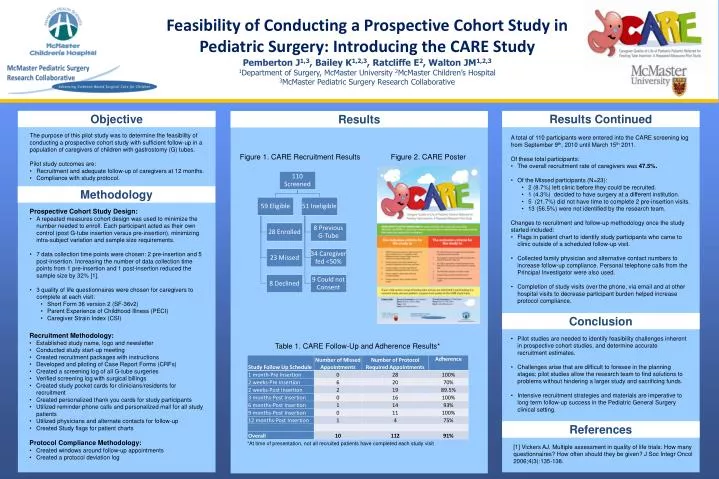
Feasibility of Conducting a Prospective Cohort Study in Pediatric Surgery: Introducing the CARE StudyPemberton J1,3, Bailey K1,2,3, Ratcliffe E2, Walton JM1,2,31Department of Surgery, McMaster University 2McMaster Children’s Hospital 3McMaster Pediatric Surgery Research Collaborative Objective Results Continued Results • The purpose of this pilot study was to determine the feasibility of conducting a prospective cohort study with sufficient follow-up in a population of caregivers of children with gastrostomy (G) tubes. • Pilot study outcomes are: • Recruitment and adequate follow-up of caregivers at 12 months. • Compliance with study protocol. • A total of 110 participants were entered into the CARE screening log from September 9th, 2010 until March 15th2011. • Of these total participants: • The overall recruitment rate of caregivers was 47.5%. • Of the Missed participants (N=23): • 2 (8.7%) left clinic before they could be recruited. • 1 (4.3%) decided to have surgery at a different institution. • 5 (21.7%) did not have time to complete 2 pre-insertion visits. • 13 (56.5%) were not identified by the research team. • Changes to recruitment and follow-up methodology once the study started included: • Flags in patient chart to identify study participants who came to clinic outside of a scheduled follow-up visit. • Collected family physician and alternative contact numbers to increase follow-up compliance. Personal telephone calls from the Principal Investigator were also used. • Completion of study visits over the phone, via email and at other hospital visits to decrease participant burden helped increase protocol compliance. Figure 1. CARE Recruitment Results Figure 2. CARE Poster Methodology • Prospective Cohort Study Design: • A repeated measures cohort design was used to minimize the number needed to enroll. Each participant acted as their own control (post G-tube insertion versus pre-insertion), minimizing intra-subject variation and sample size requirements. • 7 data collection time points were chosen: 2 pre-insertion and 5 post-insertion. Increasing the number of data collection time points from 1 pre-insertion and 1 post-insertion reduced the sample size by 32% [1]. • 3 quality of life questionnaires were chosen for caregivers to complete at each visit: • Short Form 36 version 2 (SF-36v2) • Parent Experience of Childhood Illness (PECI) • Caregiver Strain Index (CSI) Conclusion • Recruitment Methodology: • Established study name, logo and newsletter • Conducted study start-up meeting • Created recruitment packages with instructions • Developed and piloting of Case Report Forms (CRFs) • Created a screening log of all G-tube surgeries • Verified screening log with surgical billings • Created study pocket cards for clinicians/residents for recruitment • Created personalized thank you cards for study participants • Utilized reminder phone calls and personalized mail for all study patients • Utilized physicians and alternate contacts for follow-up • Created Study flags for patient charts • Protocol Compliance Methodology: • Created windows around follow-up appointments • Created a protocol deviation log • Pilot studies are needed to identify feasibility challenges inherent in prospective cohort studies, and determine accurate recruitment estimates. • Challenges arise that are difficult to foresee in the planning stages; pilot studies allow the research team to find solutions to problems without hindering a larger study and sacrificing funds. • Intensive recruitment strategies and materials are imperative to long term follow-up success in the Pediatric General Surgery clinical setting. Table 1. CARE Follow-Up and Adherence Results* References *At time of presentation, not all recruited patients have completed each study visit • [1] Vickers AJ. Multiple assessment in quality of life trials: How many questionnaires? How often should they be given? J SocIntegrOncol 2006;4(3):135-138.