Download
1 / 27
270 likes | 316 Views
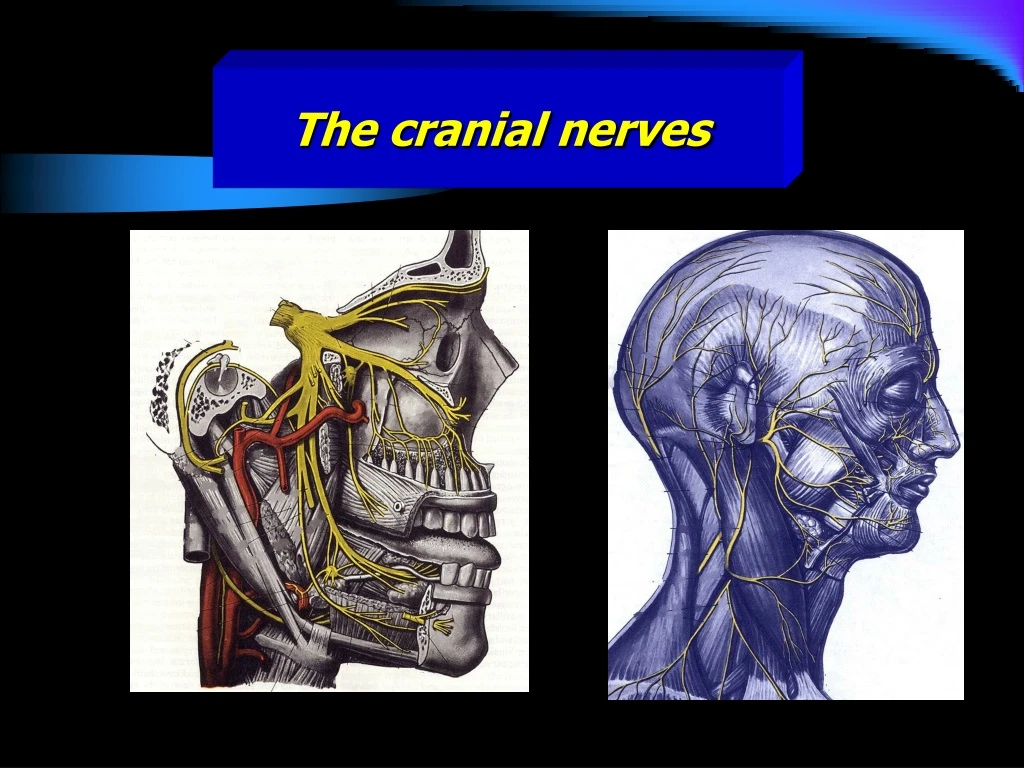
The cranial nerves. The cranial nerves. These are twelve pairs and numbered from before backward. All the nerves are distributed in the head and neck except the tenth which supply structures in the thorax and abdomen. Sensory: 1 st , 2 nd and 8 Th . Motor:

E N D
The cranial nerves • These are twelve pairs and numbered from before backward. • All the nerves are distributed in the head and neck except the tenth which supply structures in the thorax and abdomen. • Sensory: • 1st, 2nd and 8Th. • Motor: • 3rd, 4th, 6th, 11th and 12th. • Mixed: • 5th, 7th, 9th and 10th.
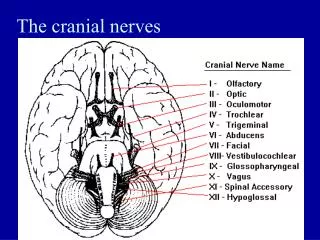
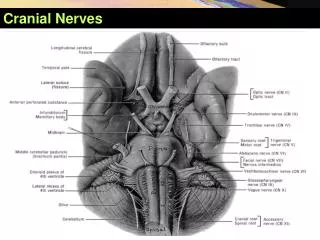
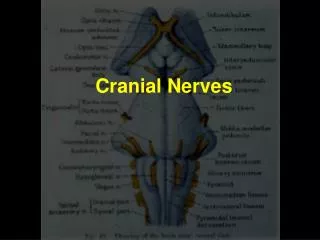
Cr I Olfactory Cr II Optic Cr III Oculomotor Cr IV Trochlear Cr V Trigeminal Cr VI Abducent Cr VII Facial Cr VIII Vestibulocochlear Cr XI Glossopharyngeal Cr X Vagus Cr XI Accessory Cr XII Hypoglossal The cranial nerves Overview
The cranial nerves • The first two are merely an outdrawn part of the CNS rather than nerves. • Olfactory: (Sensory) Cr I • Optic: (sensory) Cr II
Olfactory:(Sensory) Cr I • Fibers originate in the upper part of the nose. • They are unique in being the central processes not peripheral ones • Clinically: • Bilateral anosmia & CSF leak • are common signs of head • injuries with anterior cranial • fossa fracture.
Optic:(sensory) Cr II • Leaves the orbital cavity through the optic canal They join each other to form the chiasma. • Clinically: • Section through the optic nerve • causes epsilateral blindness. • Lesions behind the optic chiasma • (pituitary gland tumors) lead to • contro-lateral blindness.
Oculomotor nerve:(motor) Cr III • Oculo: Eye + Motor: mover • Somatic nerve to four of the six muscles of that moves the eye and the muscle that raises the eyelids • Enter the orbit through superior orbital fissure
Oculomotor nerve:(motor) Cr III • Clinically: • Inability to look up, down or medially. • Dilatation of the pupil. • Ptosis (drooping of the eyelid paralysis • of LPS) • Supply all the orbital muscles, except the superior oblique,lateral rectus and levator palpebrae superioris • Supply parasympathic fibers to the constrictors of the pupil.
Trochlear nerve: (motor) Cr IV • Enter through the superior orbital fissure • supply the superior oblique muscle • Clinically: • Unable to look downward and • inward. • Difficulty in walking downstairs
Trigeminal Nerve: (mixed) Cr V • Motor nucleus (branchial) in the upper pons, for the muscles of the first branchial arch. • Sensory nucleus (somatic) divided into three • Mesencephalic • Main • Spinal
Trigeminal Nerve: (mixed) Cr V • Mesencephalic: • extend through the midbrain • First order neurons • mediate proprioceptive impulses • Main sensory: • upper pons lateral to the motor • second order neurons • mediate touch • Spinal: • extend from lower pons, medulla to spinal cord • second order neurons • mediate pain & temperature
Trigeminal Nerve: (mixed) Cr V • Ophthalmic division: • It is the nerve for the frontonasal process • emerging through the superior orbital fissure • divide into three branches: 1-Lacrimal nerve. 2-Frontal nerve. 3-Nasociliary nerve.
Trigeminal Nerve:(mixed) Cr V • Maxillary division: • It is the nerve to the maxillary process, leaves the skull through foramen rotundum and have a very short course. • Ganglionic branches • zygomatic nerve • posterior superior alveolar nerve • Infraorbital nerve
Trigeminal Nerve: (mixed) Cr V • Mandibular division: • It is the nerve for the first pharyngeal arch, very short and emerges through foramen ovale • Accompanied by the motor root of the trigeminal nerve • divide into: • Anterior division • all motor except one • Posterior division • all sensory except one
Trigeminal Nerve: (mixed) Cr V • Nerve to medial pterygoid muscle • Anterior branches: • nerves to lateral pterygoid, masseter and two deep temporal • the long buccal nerve “S”. • Posterior branches: • Auriculotemporal • inferior alveolar (nerve to mylohoid “M”) • the lingual nerves
Trigeminal Nerve: (mixed) Cr V • Clinically • Fracture midface, zygoma or mandible might lead • to anaesthesia to light touch and other modalities. • Lesions of the entire nerve leads to • anaesthesia and paralysis and atrophy • of the muscles of mastication. • Trigeminal neuralgia • Herpes zoster
Abducent :(motor) Cr VI • Somatic, leave the brain through the superior orbital fissure • Supply the lateral rectus muscle. • Clinically: • Strabismus and diplopia • on lateral gaze
Facial:(mixed) Cr VII • Joined by the nervus intermedius, sensory root, in the facial canal in the temporal bone before it emerges through the stylomastoid foramen. • Passes into the parotid gland and divides into five motor • Branchial motor branches: • supply the muscles of the facial expression (from second pharyngeal arch)
Facial:(mixed) Cr VII • Visceral efferent: • Secretomotor to submandibular & sublingual salivary gland • Sensory fibers: • Visceral afferent • Taste buds anterior two third of tongue & soft palate • Somatic afferent • skin of external auditory meatus and tympanic membrane • Clinically: • Bell’s Palsy • Loud sound, • paralysis of stapidus muscle
Vestibulocochlear:(sensory) CrVIII • A special sensory nerve, consist of two kinds of fibers, the vestibular and the cochlear • Mediate sound reception and balance. • Clinically: • Deafness • vertigo
Glossopharyngeal Nerve:(mixed) Cr IX • Sensory: • Special: • taste from the posterior 1/3 of tongue. • General sensation: • from the back of the tongue wall of the pharynx and the middle ear. • Chemoreceptor & pressure: • Carotid sinus concerned with regulation of respiration and circulation
Glossopharyngeal Nerve:(mixed) Cr IX • Motor: • To the stylopharyngeus muscle of the pharynx. • Parasympathetic fibres: • to the otic ganglion, the postganglionic fibres travel with the auriculo-temporalnerve to the parotid • Clinically: • Neuralgia. • Loss of gagging reflex
Vagus nerve:mixed Cr X • Has the most extensive distribution of all the cranial nerves, supply the heart and the major part of the respiratory and alimentary tract. • Has one sensory and two motor nuclei in the medulla. • Leave the cranial cavity through the jugular foramen. • passes vertically down the neck within the carotid sheath.
Vagus nerve:mixed Cr X • Have 4 types of fibres: • Motor fibres to the striated muscles of larynx and pharynx. • Paralysis of soft palate, dysphagia and aphonia • Visceral-motor fibres carry impulses to thoracic and abdominal viscera • Sensory fibres • for pain from external auditory meatus • Visceral fibres: • Taste buds in the epiglottis • Stretch receptors in the heart, aorta and common carotid bifurcation (Blood Pressure and heart rate) • Stretch receptors in the lung and upper G-T I (rate and depth of respiration
Accessory nerve:(Motor) Cr XI • A small cranial root which is distributed to the muscles of the palate, pharynx and larynx. • A large spinal root to the sternocleidomastoid and trapezius muscles.
Accessory nerve:(Motor) Cr XI • Clinically: • Paresis of the laryngeal and pharyngeal muscles leading to dysphonia and dysphagia. • Paresis of the trapezius and sternocleidomastoid muscle following neck dissection for tumour surgery.
Hypoglossalnerve:(Motor) Cr XII • Leave the posterior cranial fossa via the hypoglossal canal in the occipital bone. • Supply the intrinsic and the extrinsic muscles of the tongue with the exception of the palatoglossus • Clinically: • Unilateral lingual paresis • hemiatrophy of the tongue • Dysarthia.