Download
1 / 22
230 likes | 764 Views
Wegener’s Granulomatosis. Jason Kidd Morning Report 11/18/2009. Wegener : Controversy.

E N D
Wegener’s Granulomatosis Jason Kidd Morning Report 11/18/2009
Wegener: Controversy “Unlike doctors who joined the Nazi Party to be allowed to practice, Wegener joined the movement in 1932, before Hitler took power. He rose to a relatively high military rank and spent some of the war in a medical office three blocks from the Jewish ghetto in Lodz, Poland. Sketchy records suggest that he might have participated in experiments on concentration camp inmates.” Feder, NY Times 1/22/2008
Definition • “A distinct clinicopathologic entity characterized by granulomatousvasculitis of the upper and lower respiratory tracts together with glomerulonephritis.” Harrison’s
Incidence and Prevalence • Estimated prevalence: 3 per 100,000 • 1:1 male to female ratio • Mean onset: 40 Harrison’s
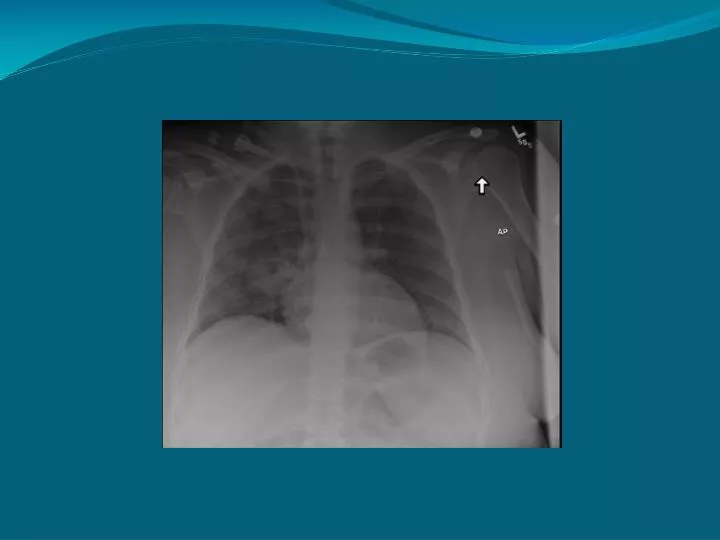
Diagnostic Criteria: • American College of Rheumatology proposed clinical criteria for diagnosis of WG: • Nasal or oral inflammation • Abnormal CXR • Abnormal urinary sediment: hematuria with or without RBC casts • Granulomatous inflammation on biopsy Adapted from UpToDate and Harrison’s
Diagnosis • According to the Chapel Hill Consensus Conference: • Granulomatous inflammation of respiratory tract • Vasculitis of small to medium size vessels Jennette JC et al, Arthritis Rheum 1994
Upper Respiratory Tract • Upper airway disease occurs in 90% of patients • Nasal involvement may present with epistaxis, rhinorrhea, purulent discharge • Otitis media and eustachian tube blockage can occur • Nasal septal perforation may occur, leading to saddle nose deformity • Subglottic tracheal stenosis can cause airway obstruction
Pulmonary Involvement • Cough, hemoptysis, dyspnea • Infiltrates and cavitary lesions can be seen on radiography • Lung involvement typically appears as bilateral, nodular cavitary infiltrates • Biopsy: necrotizing granulomatousvasculitis
Renal Involvement • Generally manifested with acute renal failure • Urine sediment: red cells, red cell casts, proteinuria • Accounts for most of the mortality of this disease • Renal biopsy: segmental necrotizing glomerulonephritis
Laboratory tests • Nonspecific • Leukocytosis, thrombocytosis, elevated CRP, elevated ESR can all be seen • 90-95% of patients with active Wegener’s are ANCA positive • Diagnosis is confirmed by biopsy at site of active disease
Other Manifestations • Joints: myalgias, arthralgias • Eyes: episcleritis, uveitis • Skin: palpable purpura, ulcerative lesions • CNS: cranial nerve abnormalities • Cardiac: pericarditis, coronary vasculitis • High incidence of DVT
Treatment • Diagnosis • Remission Induction • Remission maintenance • Relapsing Disease • Refractory Disease
Remission Induction • Glucocorticoids • Dosing has not been examined in randomized trials • Generally start 1 mg/kg/day10-20 mg daily at 12 weeks • Cyclophosphamide • Pulsed, IV is thought to be safer then oral • Risk of myelosuppresion, infection, malignancy • Plasma Exchange • Shown in small studies to improve chances of renal recovery • Recommended in lung hemorrhage Jayne, Nephrology 2009
Remission Maintenance • Azathioprine or Methotrexate can be substituted for Cyclophosphamide after 3-6 months • No standard length of treatment or regimen • Relapses occur mostly in pt’s with continued ANCA positivity • Relapse in WG has been assoc with nasal carriage of S. Aureus • Utility of TMP/SMX prophylaxis? Jayne, Nephrology 2009
What happened? • She received IV Cytoxan and Plex while hospitalized • She has received a total of 3 doses of IV Cytoxan • BAL grew Penicillium, currently being treated w/Vori • She developed LE petechiae and RLE DVT • She continues to be HD dependent
Sources • Carruthers D et al, Evidence based management of ANCA vasculitis, Best Practice & Research Clinical Rheumatology 2009, 23:367-378 • Feder B, A Nazi Past Casts a Pall on Name of Disease, New York Times, Jan 22 2008 • Jayne D, Progress of treatment in ANCA-associated vasculitis, Nephrology 2009, 14: 42-48 • Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL, Hagen EC, Hoffman GS, Hunder GG, Kallenberg CG, et al. Nomenclature of systemic vasculitides. Proposal of an international consensus conference. Arthritis Rheum 1994;37:187-92 • Jennette JC, Falk RJ, Small Vessel Vasculitis, New England Journal of Medicine, 1997, 21: 1512-1523 • Kasper et al, Harrison’s Principles of Internal Medicine, 2005 • UpToDate 2009