Download
1 / 51
510 likes | 770 Views
Mitral Valve Prolapse and Regurgitation. Jason Infeld, MD, FACC Stern Cardiovascular Foundation. DISCLOSURE. Jason Infeld MD, FACC Stern Cardiovascular Foundation I have the following personal financial relationships with commercial interests to disclose: NONE. Mitral Valve Prolapse (MVP).

E N D
Mitral Valve Prolapse and Regurgitation Jason Infeld, MD, FACC Stern Cardiovascular Foundation
DISCLOSURE Jason Infeld MD, FACC Stern Cardiovascular Foundation I have the following personal financial relationships with commercial interests to disclose: NONE
Mitral Valve Prolapse (MVP) • MVP is the most common cause of mitral regurgitation and of congenital valvular heart disease in adults • Definition and diagnostic criteria have changed leading to significant controversy • Many common perceptions about this disease have been recently been shown to be false • Disease was widely overdiagnosed in the 70’s and 80’s as echocardiography became more widely available
What is MVP? • Systolic bowing of one or both mitral valve leaflets across the plane of the mitral valve annulus into the LA • Disease is often benign, but may be associated severe complications including mitral regurgitation, endocarditis, and arrythmias.
Classic Mitral-Valve Prolapse during Systole Freed L et al. N Engl J Med 1999;341:1-7
Classic Mitral-Valve Prolapse with Leaflet Thickening (Arrows) during Diastole Freed L et al. N Engl J Med 1999;341:1-7
How common is MVP? • Early prevalence estimates between 5 and 20% and up to 35% in some studies • Disease was thought to be more common in young women • Studies were faulty due to severe selection bias and a lack of clear echocardiographic criteria
History of MVP • Described accurately in the 60’s by Barlow in a group of patients with midsystolic clicks and mitral regurgitation seen during cardiac catheterization. Diagnosis was rare. • 1970 – first description of M-mode echocardiographic findings. • Echo led to sudden dramatic increase in the diagnosis of this entity • Early studies shows prevalence as high as 35% • “Mitral valve fiasco”
History of MVP • 1980’s widespread use of 2-dimensional echo • Use of apical 4-chamber view continued to lead to significant overdiagnosis • 1987 – study published demonstrating the normal shape of the mitral valve as a “saddle” and that the 4-chamber view should not be used to make the diagnosis
Prevalence • Framingham study - prevalence approximately 1.1% • Reviewed echos of 3591 men and women • 5 to 1 ratio of self-reported diagnosis of MVP and echocardiographic MVP • Prevalence equal between men and women • MVP patients were thinner and had more MR • Average amount of MR was trace to mild
Echocardiography Apical4-chamber view ParasternalLong-axis View
Leaflet displacement • Greater than 2mm above the plane of the mitral annulus in the parasternal long-axis view • Leaflet thickening • Greater than 5mm in the midportion of the anterior mitral leaflet
Echocardiography • Classical vs. nonclassic MVP • >2mm displacement and >5mm thickness are considered to have classic MVP • Patients with leaflet thickeness <5mm have nonclassic MVP • Symmetric vs Asymmetric prolapse
Diagnostic Pitfalls • Non-specific echo findings • M-mode • Apical 4-chamber view • Physical exam. Midsystolic clicks are common in normal individuals. • Symptoms: non-specific with significant overlap with other disease processes
Natural History of MVP • MVP is generally benign, but serious complications do occur • Complications of MVP are infective endocarditis, cerebrovascular accidents, atrial fibrillation, the need for mitral valve surgery, and death • Complication rates are between 1 and 4% annually • Complication rates vary amongst studies due to referral bias of the most serious cases to tertiary centers and maybe lower than reported • Complications can be predicted by understanding simple risk factors
Complications • Primary risk factors(RFs) for complications • Moderate to severe MR • EF less than 50%
Complications • Secondary risk factors • Slight MR • Left atrial dimension > 40 mm • Flail leaflet • Atrial fibrillation (AF) • Age >50 years.
2006 ACC/AHA Guidelines • Repeat echocardiography at yearly intervals in patients with high-risk findings on the initial echocardiogram (eg, diffuse thickening of the mitral leaflets and redundancy), or moderate MR. • Clinical evaluation and repeat echocardiography every 6 to 12 months in patients with severe MR • Clinical evaluation and echocardiography at any time there is a change in signs of symptoms.
Endocarditis Prophylaxis • The 2007 American Heart Association (AHA) guideline for the prevention of infective endocarditis made major revisions to the 1997 AHA guideline. • MVP with mitral regurgitation is no longer considered a high risk valve lesion and prophylaxis is no longer recommended. • Although MVP is associated with an increased risk of endocarditis, there are no convincing data that antibiotic prophylaxis is effective in preventing episodes of endocarditis
Chronic Mitral Regurgitation • Most patients asymptomatic even with severe MR • Progressive dilatation of the LA and LV. • LA enlargement may result in atrial fibrillation • Moderate to severe MR may eventually result in LV dysfunction and development of CHF • Pulmonary hypertension may occur with associated right ventricular dysfunction. • Typically prolonged asymptomatic interval • Maybe an accelerated phase as a result of ruptured mitral valve chordae leading to progressive left atrial and LV dysfunction and atrial fibrillation
Goals of Treatment • Prevent irreversible LV dysfunction, pulmonary HTN, or atrial fibrillation in an asymptomatic patient • Relieve symptoms of dyspnea and fatigue in symptomatic patients • Prevent sudden cardiac death
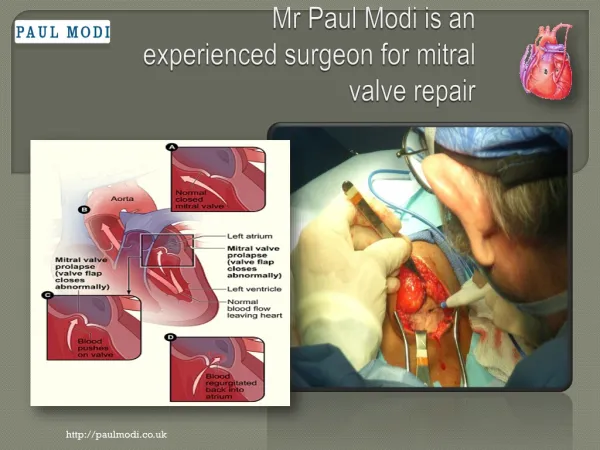
Mitral Valve Repair • Ideal treatment for mitral regurgitation. • Avoids need for anticoagulation and long-term risks of valve prosthesis • Preserves mitral valve anatomy leading to better post-operative LV function and survival • Repair is surgeon specific and success is highly correlated with volume
Mitral Valve Repair • Clinician needs to be able to determine the likelihood of repair • Isolated posterior leaflet prolapse more amenable to repair • Presence of severe anterior leaflet prolapse, severe valve thickening and calcification make repair less likely • TEE is recommended pre-operatively to define pathology and mechanism of MR
Flail Mitral Leaflet • Subset of patients who do clinically worse even in the absence of progressive LV dilatation or dysfunction. • Higher-risk of sudden cardiac death • Referral for early surgical treatment if valve amenable to repair.
TEE • Plays an important role in the evaluation of MR due to the proximity of the TEE probe to the LA • TTE can underestimate MR due to shadowing from calcification and prosthetic valves • Defines mechanism and severity of MR • Ideal test to assess if repair is feasible