Download

1 / 33
330 likes | 532 Views
A Hospital-Specific Quality Improvement Initiative for Prophylaxis of VTE in Surgical Patients. Presenters. Katherine Grichnik, MD, MS Duke University School of Medicine grich002@mc.duke.edu Scott Weber Med-IQ, LLC sweber@Med-IQ.com. Disclosures. Katherine Grichnik, MD, MS

E N D
A Hospital-Specific Quality Improvement Initiative for Prophylaxis of VTE in Surgical Patients
Presenters Katherine Grichnik, MD, MS Duke University School of Medicine grich002@mc.duke.edu Scott Weber Med-IQ, LLC sweber@Med-IQ.com
Disclosures • Katherine Grichnik, MD, MS • No relevant disclosures • (PELI [business], Inventive Medical [echocardiography]) - unrelated • Scott Weber • No relevant disclosures
Who We Are – Duke University School of Medicine Building Partnerships, Transforming Knowledge, Closing Quality Gaps
Who We Are – Med-IQ Mission To deliver education that brings measurable change in healthcare professional competency with the goal of improving performance and patient outcomes Accreditation Council for Continuing Medical Education (ACCME) Exemplary compliance Element 2.2—Needs Assessment Element 2.5—Program Evaluation Accreditation Council for Pharmacy Education (ACPE) California Board of Registered Nursing (CBRN)
Background Duke and Med-IQ: extensive experience educating physicians and nurses in VTE prophylaxis 20+ activities in VTE in the previous 3 years Focus: risk assessment and ACCP guideline adherence Consistent Level 3 and 4 outcomes Gaps still remained in quality of patient care Data analysis from current activities, plus in-practice research, reveals that knowledge/competency-based education is necessary, but insufficient Quality improvement (QI) training enhances the application of education
Data / Experience Hypothesis Activity Design Activity Evaluation Quality Improvement Process Confirm Hypothesis?
Hypotheses • Performance improvement better achieved and sustained with institutional culture of quality and safety • Education AND training core elements for clinical and process change • Clinical education that also addresses system and cultural-based barriers promotes improvements in knowledge, competency, performance change, institutional change and patient outcomes • Crew Resource Management is unique in its applicability to the surgery setting: many parallels between the OR and airline cockpits
Eastern 401 Crash http://www.youtube.com/watch?v=ICqPGkto3Yo
Crew Resource Management • A behavioral protocol • Enhances clinical leadership, situational awareness and team communication • Aviation’s first 100 years • Technological plateau of the late 60’s • New safety advancements couldn’t stop fatalities • FAA mandated in the late 1980’s to prevent accidents due to “human factors”
Aviation Safety Tools • Crew Resource Management (CRM)/Leadership Training • Briefings/Debriefings • Checklists • Standard Operating Procedures (SOPs)/Protocols • Aviation Safety Reporting System (ASRS) • Simulation
Communication Orientation/training Patient assessment Staffing Availability of info Competency/credentialing Procedural compliance Environ. safety/security Leadership Continuum of care Care planning Percent of 2966 events Organization culture 0 10 100 20 30 40 50 60 70 80 90 Applicable to Healthcare? Cause Attributed to Adverse Event (All categories; 1995-2004) Source: JCAHO Sentinel Event Statistics, 2004
Background • Citrus Memorial Hospital, Inverness FL • 198 beds, 4,000+ surgeries/year • 80% VTE prophylaxis compliance (SCIP) • Pre-activity meetings created institutional buy-in • Kick off: emphasized expectations, roles, responsibilities • Leadership: CEO, CMO, CNO and QI Director • Strategic assessment of OR communication • Follow-up care and monitoring • Surveys, interviews, focus groups, surgery observations
Background – cont. • Duke University School of Medicine • Clinical content development and program creation • Certification • MedIQ • Program creation, implementation, monitoring and follow-up • Unrestricted grant support: • Ortho-McNeil-Janssen Pharmaceuticals Scientific Affairs, LLC and Sanofi-Aventis U.S.
Activity Design • Strategic Assessment via Chart Abstraction • Assess VTE performance measures • Faculty review and observation • Hospital policies and protocols used for VTE prophylaxis in surgical patients • Specific institutional barriers to optimal VTE prophylaxis
Activity Design • Core measures: Used ACCP Guidelines • VTE prophylaxis was given when indicated? • Appropriate drug regimen used? • Timing of prophylaxis appropriate (unknown cases considered “no”)? • Duration of inpatient prophylaxis? • Discharge VTE prophylaxis ? • Overall: All guidelines met (measures 1-5)
Educational Strategy • 5-hour, onsite training sessions • 160 attendees (Entire healthcare team) • Separate tracks • MDs • Nurses/surgery techs/pharmacists • Case-based clinical exercises • Utilizing new language and protocols • Teamwork/ collaboration • VTE clinical context
Results Confidence / Knowledge / Competency
Results Performance
Performance Data • 100 charts were pulled at “A” and “C” time points • 13 charts excluded due to unclear guidelines for a particular patient • Final sample of 87 “A” charts and 66 “C” charts • Chi square tests performed • All measures with statistically significant improvement
Results Institutional Change
Hospital Stakeholders Feedback • “Much better awareness about the need to properly execute timeouts before surgeries” • “Surgeons are approaching 100% compliance on either conducting the timeouts or, at a minimum, they are initiating them. This is markedly different than before the program was presented....physicians used to expect to start cutting immediately upon entry to the OR.” • “Also much better awareness and compliance among the physician and staff about the need to appropriately prophylax.” • “While awareness and compliance with CRM principles has increased, there is less persistence in the use of CRM language. This points to the need for a more long-term program with educational reinforcement in the future.” *As described by the Director of Perioperative Services, Citrus Memorial Hospital
Hospital Stakeholders Feedback • “Before, surgeons were ambivalent about how the timeouts were done and they had less of a focus on VTE prophylaxis -- before the focus much of the time was on the use of SCDs and was the extent of prophylaxis. That is no longer the case.” • "As a result of the program, I’m no longer worried about a Joint Commission inspection or the possibility of a wrong-site surgery." *As described by the Director of Perioperative Services, Citrus Memorial Hospital
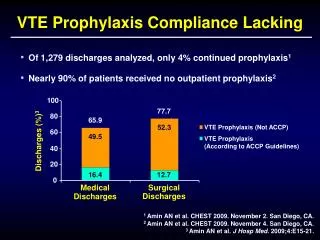
Caveat SCIP data incomplete: It does not measure that guideline-based prophylaxis is being followed—only that some form of prophylaxis is being ordered.
3 Keys to Success Unique design and intensity of CRM content was engaging Accelerated adoption of key points Education and training integrated in a clinical context VTE Framed as a safety issue not a clinical choice Hospital administration support critical It was a REQUIRED program
The Future Need extensive follow-up training to insure that all safety protocols (CUS language, SBAR communication) persist. Targeting multiple hospitals for concurrent training would allow for economy of scale Multi-dimensional analysis of outcomes data reveals provider and institution level insights
Hypotheses - revisited • Individual performance improvement can be better achieved and sustained within an institutional culture of quality and safety • Education AND training are the core elements in clinical and process change • Integrating clinical education that also addresses system and cultural-based barriers improves the chances of achieving improvement in knowledge, competency, performance change, institutional change and patient outcomes • Crew Resource Management is unique in its applicability to the surgery setting due to the parallels between the O.R. and airline cockpits
Contact Scott Weber, CEO Med-IQ, LLC 203-762-0588 sweber@med-iq.com Katherine Grichnik, MD Medical Director Duke Clinical Research Institute 919-401-1203 grich002@mc.duke.edu