Download
1 / 26
270 likes | 294 Views
Learn about types, advantages, and disadvantages of cohort studies, including famous examples and the case-cohort design. Understand the study base, population at risk, and sampling strategies used in cohort studies.

E N D
COHORT STUDIES Nigel Paneth
TYPES OF COHORT STUDIES A. TIMING B. SAMPLING C. POPULATION BASE D. OPEN AND CLOSED COHORTS
TIMING • PROSPECTIVE (OR CONCURRENT) • RETROSPECTIVE (OR NON-CONCURRENT)
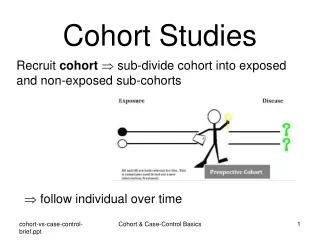
SAMPLING • cohort studies with sampling unrelated to exposure (common) • cohort studies with exposure-based sampling (rare)
POPULATION BASE • Population-based • not-population based
OPEN AND CLOSED COHORTS • OPEN - people moving in and out • CLOSED - fixed population
ADVANTAGES OF COHORT STUDIES 1. Can assess several outcomes 2. Time-order generally clear 3. Prospective control over exposure and outcome measurement possible (in prospective studies) 4. Somewhat less potential for bias than case-control studies, but equal potential for confounding
DISADVANTAGES OF COHORT STUDIES 1. Generally require large samples 2. Not useful for rare outcomes 3. As an observational study, can never be assumed to be free of confounding and bias 4. Must usually control for potential confounding in the analysis, though can control in the design
STUDY BASE IN COHORT STUDIES • The study base is the person-time experience of the individuals in whom the outcome is ascertained. • Study base should be the same for exposed and unexposed in cohort studies. Thus the denominator for calculation of incidence rates must be the same number of people for the same period of observation. • Calculation of person-years at risk is the means of achieving equivalence of study base in cohort studies.
POPULATION AT RISK IN COHORT STUDIES 1. At baseline, we start with a cohort free of disease 2. If analysis is by cumulative incidence, then denominator is study population at baseline. 3. If analysis is by incidence density, then denominator is person-years at risk.
FAMOUS COHORT STUDIES • POPULATION-BASED • CARDIOVASCULAR • CHILD HEALTH • SPECIAL EXPOSURES • NON-POPULATION BASED • OCCUPATIONAL – for convenience • OCCUPATIONAL – to study the occupation • HEALTH CARE SETTINGS • VETERANS
1. CARDIOVASCULAR DISEASE • Framingham, MA • Tecumseh, MI • Evans county, GA (biracial) • Muscatine, IA • Bogalusa, LA (children)
2. CHILD HEALTH • National Birthday Trust Studies One week of births in England and Wales in 1946, 1958 and 1970 • Project on Premature Infants All births < 1,500 g or < 32 weeks in Holland in 1983 • The National Childrens Studyhttp://www.nichd.nih.gov/about/despr/despr.htm Will we shortly begin a study in the US of 100,000 pregnancies with offspring followed to age 21?
3. SPECIAL EXPOSURES • Atomic Bomb Casualty Commission (ABCC): Hiroshima and Nagasaki survivors (effects of radiation) • Dutch famine survivors (effects of starvation) • Seveso (effects of dioxin exposure)
1. OCCUPATION-BASED COHORTSBECAUSE OF CONVENIENT FOLLOW-UP • British Doctors Study (Doll – smoking) • Nurses Study (Speizer, Willett – many issues) • London civil servants (Marmot - SES) • Taiwanese civil servants (Beasley – liver cancer)
2. OCCUPATION BASED TO STUDY EXPOSURES • Benzene-workers (leukemia) • Coke-oven workers (lung cancer) • Asbestos workers (lung cancer) • Radium dial painters (oral cancer)
3. SAMPLING FROM HEALTH CARE SETTINGS • National Collaborative Perinatal Project: Almost all pregnancies at 12 medical centers 1959-1966 – N about 50,000. (causes of CP) • Child Health and Development Studies: Kaiser-Permanente births (many issues) • Patients treated with radiation for polycythemia or ankylosing spondylitis (radiation and cancer)
4. VETERANS • Mustard-gas poisoning from WW I (lung disease) • Vietnam Veterans (post-traumatic stress disorder, agent orange effects) • Gulf War Veterans (Gulf war syndrome)
CASE-COHORT DESIGN: PURPOSE The case-cohort design is used to reduce the costs of exposure assessment
CASE-COHORT DESIGN: APPROACH 1. A population at risk is identified and screened for disease, and prevalent cases are omitted. 2. A case-identification procedure is developed to detect new cases of disease in the cohort. (so far all is the same as any cohort study)
CASE-COHORT DESIGN: APPROACH 3. The whole cohort is subject to case-identification, but only a random sample (called the sub-cohort) receives detailed exposure assessment. 4. The cases are those emerging in the population (both in and out of the sub-cohort); the controls are subjects in the sub-cohort who are not cases. 5. Analysis is like a cohort study. Since the sampling fraction is known, and the entire population is sampled for caseness, true incidences and relative risks can be calculated.