Download
1 / 33
340 likes | 538 Views
PROTEL, A FEASIBILITY STUDY. EXPERIMENT PROTEL (PROtoni TErapia Locale). 2 years Padova (C.N. P. Rossi) LNL (R.L. G. Moschini) Pavia ( D. Scannicchio) parteciperà nel secondo anno

E N D
PROTEL, A FEASIBILITY STUDY EXPERIMENT PROTEL (PROtoni TErapia Locale). 2 years Padova (C.N. P. Rossi) LNL (R.L. G. Moschini) Pavia ( D. Scannicchio) parteciperà nel secondo anno 1)PROTEL is a feasibility study of an innovative nuclear device to perform local proton radiotherapy for brachytherapy and IORT* like applications. The device would exploit the nuclear reaction 2H(3He,p)4He to obtain high energy protons (17 MeV), starting from low energy 3He ions (800 keV). These latter may be produced by a low cost portable compact accelerator adequate for hospital usage. 2)PROTEL would provisionally use the existing LNL-AN2000 accelerator 3He ions for assessing the therapeutic adequacy of this kind of proton radiation and testing key parts of the future device. Moreover PROTEL would offer a conceptual design of a compact future accelerator and a recommendation on the actual usage of this method. (*IORT: Intra Operative Radio Therapy) `
Scientific Basis Nuclear Instruments and Methods in Physics Research B 106 (1995) 606-617 The use of low energy, ion induced nuclear reactions for proton radiotherapy applications KM. Horna* , B. Doyle a, M.N. Segal b, R.W. Hamm c, R.J. Adler d, E. Glatsteine a Sandia National Laboratories. USA b Department of Otolaryngology, UniLersity of New Mexico Medical School. USA C Accsys Technology Inc., USA d North Star Research Corp., USA e Department of Rad. Oncology, Universiiy of Texas Southwest Medical Center. USA p(17.4 MeV) Needle for Radiotherapy 10 mA Low energy RFQ 3He(0.8 MeV) TiD2 (5-10 mm) Reaction 2H(3He,p)4He No industrial realization followed this idea
Scientific Basis - 2 Later (2005), K.L. Leung and coll. of the Lawrence Berkeley National Laboratory (LBNL) (CA, USA) proposed to employ a portable ion tube accelerator extremely light and compact (few kilos, 20-30 cm), being operated at a much lower energy (~ 150 keV). This device is designed to produce 3He ions in a plasma chamber and then extract a 3He ion beam. It accelerates the beam down a thin hollow tube to hit a deuteron-bearing target. However, they did not demonstrate the feasibility of this device, and no prototype has been made. Actually the reaction cross section at 150 keV 3He is depressed by 20 times with respect to maximum and the required proton intensity looks difficult to obtain. To my knowledge, both teams at Sandia and Berkeley have no further plans to develop this device.
Why suggest again this method? • We have today cheaper and lighter compact accelerator that may render easier and cheaper the hospital usage of this device • Potential medical application look today more fashionable (IORT for breast cancer) • The Sandia study has not exhausted in detail all the medical possible applications and the related configuration of the aiming system • Other non-medical application look possible (rad-hard microchip assessment,…) that have not been considered • We can easily reproduce, with the AN2000 for test purposes, the nuclear reaction that give rise to the intermediate energy protons (17 MeV)
The cross section of 2H(3He,p)4He (EXFOR) NO gamma and neutron background for 3He with E < 1 MeV
Doses in H2O in f(r) from a p(17 MeV) point-like source 3He current = 1 mA
Dose on tissue Metal matrices such as Ti, Zr, Er, Sc, maintain stable H or 2H concentration. D in Ti may reach a stoichiometry of TiD2 ( c= 1.16·1023 cm-3). The cs of 2H(3He,p)4He has a broad peak at 650 keV, high s=825 mbarn. To consider the energy loss in the target and maximize the yield, the impinging3He should have ~ 800 keV. Total Integrated cs over its full range of 1.9 in TiD2 is Is=∫dz · s(E(z)) · exp(-mz) = 6.7·10-19 cm3. N=number of incident 3He atoms= Qtot/e = 6.25·1012 · Q(mC) Y=Yield= N ·c ·Is = 4.85 · 107 ·Q(mC) The average dose (every p looses between 13.6 and 17.4 MeV on a sphere of 3.1 mm) is ~ 1 Gy · Q(mC).
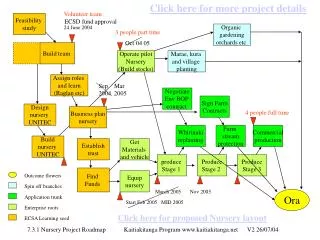
Goals and Schedule 1)Development of an experimental setup to evaluate the nuclear reaction 2H(3He, p)4He. We will employ a 3He beam of LNL vdg AN2000. The setup includes detectors for measuring the energy spectrum and the angular distribution of the ions, both 3He and p (1st year, Padova, LNL) 2) Acquisition of a deuterated target, like, for example, TiD2 and development of the 3He needle-like aiming system that includes the target by the end tip. Feasibility study of a multiple needle aimimg system. (1st year, Padova) 3) Evaluation of the effectiveness of the needle and the alignment of 3He with it . Measurement of the emitted protons intensity and shape. Evaluation of dose and damage on phantoms to a high precision, by applying micro-dosimetric methods. (1st-2nd year, Padova, LNL, Pavia) 4) Theoretical assessment of the therapeutic adequacy of the produced protons for local radio-therapy as for energy (17 MeV), intensity and emission shape, by doing numeric simulations and tests on phantoms at the AN2000 setup. The assessment will also be based on a bibliographic research and the experience of medical staff (2nd year, Pavia, LNL, Padova) 5) We will “conceptually” design, but not realize, a compact device to be employed in hospital environment. The design will include ion source, accelerator, the steering system to convey the He-3 ions, and the aiming system. It will also include assessment of industrial feasibility, cost, and radio-protection issues related to hospital usage. (2nd year, Padova, LNL, LNL-Gruppo Macchine?) 6) We will compare the device to other existing solutions, and offer a final recommendation on its actual usage and development by a manufacturer.(2nd year, Padova, LNL, Pavia)
Costi (Consumo) Padova -lavorazioni meccaniche esterne per ago deuterato -preparazione bersaglio di TiD2 -materiali meccanici LNL -adattamento linea microfascio e camera di scattering -rivelatore per protoni ad energia intermedia e adattamento readout -contributo bottiglia 3He (intiera 35000 € )
Setup adjustment and test at the AN2000 (LNL, PD) p(17 MeV) 50 nA 3He (800 keV) Scattering chamber Microbeam (0°) or chamber at (60°) -Scattering chamber adjustment for in-air irradiation with needle, including flange, detector and goniometer -Study of the effectiveness of the needle with deuterated tip
Conceptual Design of a portable system, for hospital usage (LNL-gruppo Macchine)
Are these protons (17 MeV, range= 3mm)really useful in Medicine? (LNL, PD, PV) The radiation cannot penetrate too much. Lets examine three cases to see potential uses and shortcomings Brachitherapy (f.e. prostate cancer) Surface irradiation (skin cancer, skin melanoma) Intra-Operative Radiotherapy (IORT, f.e. breast cancer)
Transport system 800 KeV He-3 Portable Accelerator (not on scale) 1)Configuration for brachytherapy-like application Patient body Needle (1.0-2.0 x 50 mm) TiD2 target irradiation area (range=3.1 mm) 17 MeV protons
1bis) Multiple Needles Brachytheraphy 800 KeV He-3 Vacuum pipe Patient body
2)Intra Operative Radio Therapy (IORT) 800 KeV He-3 800 KeV He-3 TiD2 target Needle (1.0-2.0 x 50 mm) Patient body Patient body 17 MeV protons 17 MeV protons irradiation area (range=3.1 mm) irradiation area (range=3.1 mm)
2bis )Large Field IORT Thin Deuterated target (5-10 mm) Thick Metallic support 800 KeV He-3 Conformal irradiation screen sector Patient body R=3.1mm 10-20 mm Field=10-20 mm irradiation area 1-2 mm
HDR temporary brachytherapy instead involves placing very tiny plastic catheters into the prostate gland, and then giving a series of radiation treatments through these catheters. The catheters are then easily pulled out, and no radioactive material is left in the prostate gland. Radioactive iridium seed into the catheters one by one.So one is able to control the radiation dose in different regions of the prostate. We can give the tumor a higher dose, and we can ensure that the urine passage (urethra) and rectum will receive a lower dose. Prostate BrachytherapyHDR (High Dose Radiotherapy) There is also the permanent seed implant (125I, X~27keV, m-1~20mm) or (103Pd, X~20keV, m-1~10mm the seeds are placed in the prostate by needles through the perineal skin (between the scrotum and the rectum) under anesthesia in an operating room environment. p17MeV range too small and needles connection stiff
Non-melanoma skin cancer The most common forms of non-melanoma skin cancer are called basal cell carcinoma and squamous cell carcinoma, reflecting the different types of skin cell from which the disease can develop. Treatment usually needs only to remove the cancer that is visible, as most non-melanoma skin cancers are unlikely to spread to other parts of the body. In some cases one type of treatment is all that is needed. Topical therapy (creams), PDT (Photodynamic Therapy) are often used. Surgery is successful for most types of non-melanoma skin cancer. There are a variety of different procedures, which doctors will select depending on the type and extent of the cancer. Doctors use radiotherapy as a treatment for non-melanoma skin cancers that cover a large area. or are in areas of the body that are difficult to operate on. It is also an alternative for people who may find surgery difficult to cope with, such as elderly people or those in poor health.
Malignant melanoma Surgery can certainly remove the original melanoma tumor and any affected lymph nodes. However, the spread of the melanoma, whether it is to the rest of the lymph nodes with Stage 3, and other organs for Stage 4, means more aggressive treatment with chemotherapy, radiotherapy and/or immunotherapies is needed. Melanoma does not respond to Radiotherapy in a predictable way. For this reason it is rarely used for treating primary melanoma but it is very occasionally used when surgery is not suitable. Radiotherapy is also used more to prevent the cancer's spread rather than provide a cure. High energy X-rays target a specific area to destroy the cancer cells. There are also indications that radio-sensibilizer chemicals may boost the effectiveness of radiotherapy in curing bthis kind of cancer Malignant skin Melanoma(3 mm range are enough?)
Malignant Melanoma -2 how much surgical removal of a margin of normal tissue is recommended for melanomas? If requirement of at least 1 cm removal means that also the radiotherapy should penetrate that much, PROTEL is ineffective, but ….
Intra-operative RadioTherapy Usually e- linac (6-12 MV) Max dose relase 10-12 mm (for e- linac)
Breast Cancer. Electron linac (LIAC)SORDINA spa, Saonara, GIO-MARCO spa (agente)
Therapy Effectiveness Conclusion PROTEL Vs Brachytherapy Confined released Dosed -rigidity of needles usage due to Beam alignment -Shorter range (3 mm) than brachy X-rays (10-20 mm) Is this really bad? PROTEL Vs IORT or surface application -Shorter range (3 mm) than IORT e- or Xrays (10 mm). Is this really bad? Confined released Dose
Other Applications possiblecheap high energy protons… For example: rad-hard microchip assessment Others??
Conclusion The nuclear reaction base of PROTEL has been considered for radiotherapy since the nineties. In spite of this, no exhaustive assessment of its therapeutic interest has been carried out. The advantages are of course the dose confinement typical of protons and the reduced cost. After 13 years since the first proposal, accelerators are even cheaper and lighter and PROTEL seems adequate to become a portable tool for surgery room and even for doctor’s office. Among the medical indications are the prostate, skin and breast cancers, where local radiotherapy (either brachytherapy like and IORT) are already indicated. The most weak facet of this method is the range of protons (3 mm in tissue) that might be too small for some of this applications. Other issues are the fragility of the vacuum window in the needle tip and of course the requirement of a perfect beam alignment that might spoil the PROTEL flexibility. Cheap 17 MeV Protons with limited intensity might find also non-medical application, like in the rad-hard microchips assessment. The LNL AN2000 vdg accelerator may easily offer now the 3He ions for provisional tests. For all these reasons, a feasibility study, employing also the AN2000, and addressing therapeutic possibilities and issues looks advisable.
Non malignant skin cancer Skin reaction during topical therapy for superficial skin cancer. Note the selective response as only skin cancer and precancerous cells are reacting. PDT (Photodynamic Therapy) applies a chemical (photosensitizer) that sensitizes your skin to light. Cancerous skin treated with this photosensitizer is then exposed to various light sources
Needles insertion Brachytherapy is a minimally invasive procedure where the doctor implants tiny permanent radioactive seeds (about the size of a grain of rice) into the prostate where they irradiate the cancer from inside the gland. The implanted seeds are small enough that they will not be felt by the patient. Depending on your circumstances, either (125I, X~27keV, m-1~20mm) or (103Pd, X~20keV, m-1~10mm ) will be used. Brachytherapy is also referred to as interstitial radiation therapy or seed implant therapy. Before the seeds are implanted, the patient receives anesthesia. Needles containing the seeds are then inserted through the skin of the perineum (the area between the scrotum and anus) using ultrasound guidance. The seeds remain in the prostate, where the radioactive material gives off localized radiation for a number of months to destroy the prostate cancer.