Download

1 / 23
250 likes | 702 Views
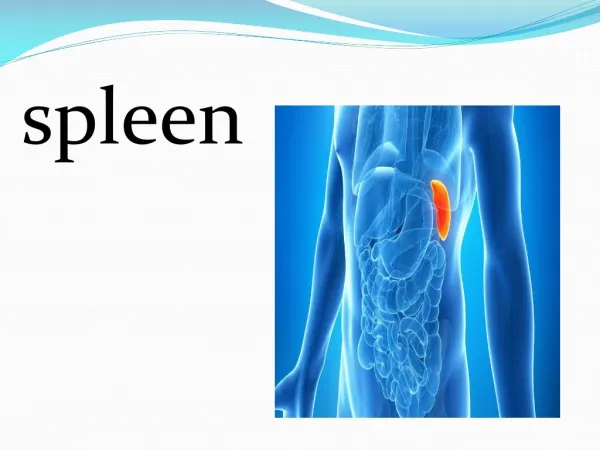
Spleen. Surface Relations Stomach Renal Colon Suspended by Phrenosplenic ligament Gastrosplenic ligament Splenocolic ligament Gastrocolic ligament Blood Supply Splenic artery, L gastroepiploic , short gastrics Splenic Vein. Anatomy. Two general components: White pulp (5-20%)

E N D
Surface Relations • Stomach • Renal • Colon • Suspended by • Phrenosplenic ligament • Gastrosplenic ligament • Splenocolic ligament • Gastrocolic ligament • Blood Supply • Splenic artery, L gastroepiploic, short gastrics • Splenic Vein Anatomy
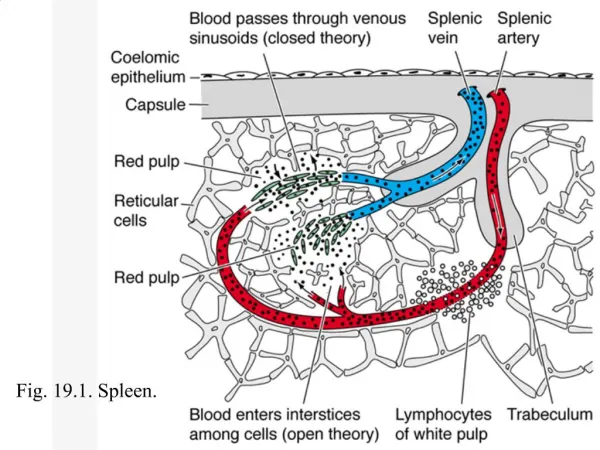
Two general components: • White pulp (5-20%) • Red pulp (~85%) • Enclosed by capsule and interspersed with trabeculae Histology
Filtration • Stiff or fragile RBCs cannot pass through interendothelial slits • Immune function • Splenic phagocytes, together with macrophages in the liver,synthesize the majority of components of the classical pathway of complement • Slow blood flow in the red pulp cords allows foreign particles to be phagocytosed without specific ligand-receptor interactions • Important in fighting early bacterial infection Physiology-for the residents!
Idiopathic thrombocytopenic purpura • Most common hematologic indication for splenectomy • Spleen is the source of circulating antiplatelet IgG • Also responsible for sequestration of sensitized platelets • Dx made by thrombocytopenia with normal bone marrow • Patients present with ecchymosis and purpura and at times there is excessive bleeding from the gums, vaginal bleeding, gastrointestinal bleeding, and hematuria • Platelet count characteristically less than 50,000/mm3 Splenectomy for platelet disorders
Idiopathic thrombocytopenic purpura • First line of treatment medical • Steroids • IgG • Plasmapheresis • Medical treatment only curative in 15% of adults • Cure rates up to 87% reported with splenectomy • Given risks of splenectomy, should be reserved for patients with platelet counts <25,000/mm3 and bleeding Splenectomy for platelet disorders
Thrombotic Thrombocytopenic Purpura • Increase of subendothelial collagen in the arterioles and capillaries causing diffuse platelet trapping • Manifested by thrombocytopenia, hemolytic anemia, fever, neurologic manifestations, and renal disease • Primarily treated with high volume plasmapheresis (80 to 90% survival) • Steroids and ASA • Splenectomy reserved for non-responders Splenectomy for platelet disorders
Hodgkin’s Disease • Historically, staging laparotomy with splenectomy were essential guides to treatment • Improvement in imaging and chemotherapy have minimized the role of the surgeon • Splenectomy for non-Hodgkin’s lymphomas • Symptomatic splenomegaly • NHL confined to the spleen or with prominent splenic involvement (survival improvement from 24 to 108 months) • Leukemias • Splenectomy indicated for symtpomatic splenomegaly Splenectomy for hematologic malignancy
Hereditary Spherocytosis • Autosomal dominant trait • Most common hemolytic anemia for which splenectomy is advised • Defective erythrocyte membrane causes trapping and disintegration within the spleen • Presents with anemia, reticulocytosis, jaundice, and splenomegaly • Diagnosis made by peripheral blood smear • Splenectomy is the only therapeutic modality (wait until age 4 to 6) • Outcomes are excellent Splenectomy for hemolytic disease
Thalasemia • Autosomal dominant transmission • Defect in the synthesis rate of hemoglobin • Thalassemia major (homozygous) presents with pallor, retarded body growth, enlarged head, and intractable ulcers • Diagnosis made by nucleated RBCs (target cells) in smear • Splenectomy reserved for patients with markedly symptomatic splenomegaly, painful splenic infarction, and increased transfusion requirement • Greater risk of post-splenectomy sepsis Splenectomy for hemolytic disease
Sickle Cell Disease • Spleen commonly enlarged during the first decade of life but then undergoes progressive atrophy due to repeated attacks of vaso-occlusion and infarction • In general, splenectomy should be avoided in patients with SCD (immunocompromized) Splenectomy for hemolytic disease
Sickle Cell Disease • Main indications are: • Acute splenic sequestration crisis • Circulatory collapse and sudden death from the rapid sequestration of red blood cells • Second-leading cause of pediatric deaths in patients with SCD • Hypersplenism • Splenectomy decreases transfusion requirements • Partial splenectomy may be an option2 • Splenic abscess • Increased incidence of Salmonella Splenectomy for hemolytic disease
The embryologic origin is in the ventral mesogastrium • The suspensory ligaments with the exception of the gastrosplenic ligament are avascular • The spleen is fixed in the LUQ and cannot be safely mobilized • Accessory spleens are most commonly located along the greater omentum With regards to splenic anatomy which of the following statements is/are true?
H. Influenzae • Strep Pneumoniae • N. Meningetidis What are the organisms that an individual must be vaccinated against to protect against OPSS?
White pulp serves a phagocytic function • Red pulp serves an immunologic function • Microcirculation is predominantly a closed system with direct AV channels • Cellular elements of the blood pass directly from red pulp cords to sinuses Which of the following is/are true regarding the microanatomy of the spleen?
The spleen can only remove cells coated with IgA • Levels of properdin and tuftsin fall after splenectomy • Lack of howell-jolly bodies after splenectomy suggests the presence of accessory spleens • Encapsulated bacteria are effectively removed in asplenic individuals • Is a site of hematopoiesis throughout life Which of the statement regarding the spleen is/are true?
Splenectomy is indicated for patients who fail to improve with initial therapy with steroids • Splenectomy is more often necessary in children with ITP than it is for adults • Splenectomy is not indicated in the absence of splenomegaly • Preoperative platelet transfusions are recommended for patients with platelets under 50K • The sole reason for splenectomy in ITP is to remove the source for platelet phagocytization Regarding the management of ITP which of the following is/are true?
Circulating antiplatelet antibodies • Venous thrombosis • Arteriolar and capillary occlusion • Intravascular activation of the coagulation cascade The primary pathophysiology of TTP involves which one of the following?
Lymphangiography and CT used together have eliminated the need for staging laparotomy • The operative technique of a staging laparotomy is different for women than men • Partial splenectomy is adequate for staging and has helped lower OPSS • Staging laparotomy results is a change in the stage of Hodgkin’s disease in 40% of cases Regarding staging laparotomy of patients with Hodgkin’s disease, which of the following statements is/are ture?
CLL • CML • Non-Hodgkin’s lymphoma • Hairy cell leukemia • Myeloid metaplasia In which of the following disorders does splenectomy clearly influence survival?
It is the most common complication of splenectomy for hematologic disease • The onset is typically characterized by sudden high fevers • It is more common in adults than in children • It is more commonly fatal in children than adults • It is more common after splenectomy for hematologic disease than for trauma Regarding Postsplenectomy sepsis, which of the following statements is/are true?