Download
1 / 56
560 likes | 600 Views
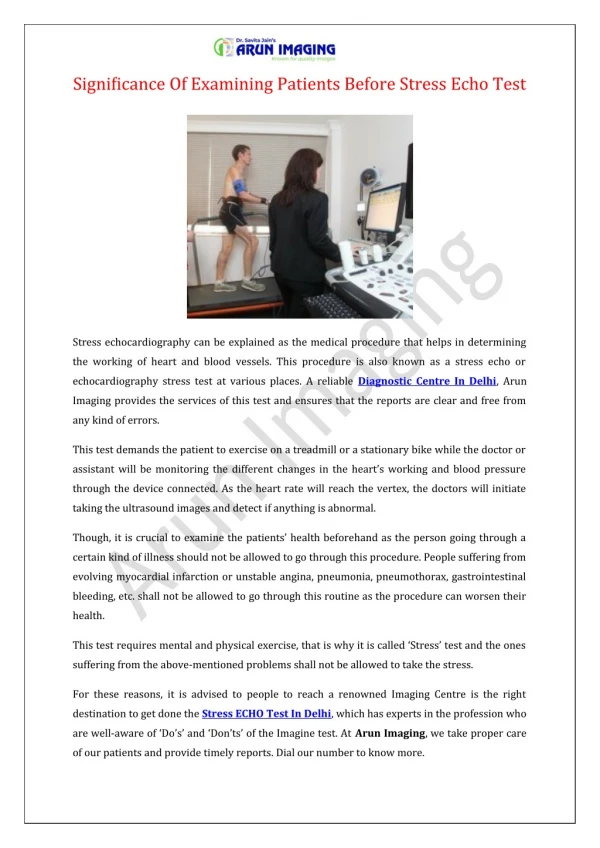
Stress echo is a family of cardiovascular stress examinations involving echocardiographic monitoring before, during, and after stress induction through exercise or pharmacological agents. Learn about coronary blood flow, coronary blood flow reserve, cellular mechanisms of ischemia, and basic principles of stress echo. Discover the differences between treadmill and supine bicycle protocols, advantages, disadvantages, indications for pharmacological stress echocardiography, and details about stress agents like dobutamine, dipyridamole, and adenosine.

E N D
STRESS ECHO DEEPAK NANDAN
Stress echo is a family of examinations in which 2D echocardiographic monitoring is undertaken before , during & after cardiovascular stress • Cardiovascular stress exercise pharmacological agents
PHYSIOLOGY • Coronary blood flow – pulsatile & phasic • Precapillary arterioles – resistance vessels * principal contributor of resistance * main controller of coronary blood flow • ↑ CBF on ↑ demand occurs through reduction in resistance at this level
CORONARY BLOOD FLOW RESERVE • Maximal CBF / basal CBF • Magnitude of bf ↑ secondary to any stress relative to resting flow • In discrete stenosis – CFR begins to ↓ when stenosis reaches 50% dm • CFR is abolished when stenosis reaches 90% • Resting bf remains constant up to 85- 90% of the stenosis
Cellular Mechanism of Ischemia • Consequence(s) of Mechanical Dysfunction • Mechanical Dysfunction • Abnormal Contraction and Relaxation • Diastolic Tension • Diastolic Wall Tension (Stiffness) Extravascular Compression Blood Flow to Microcirculation ( O2 delivery to Myocytes) O2 Consumption (to maintain tonic contraction) ATP Hydrolysis O2 Demand O2 Supply Modified from: Belardinelli et al. Eur Heart 8 (Suppl. A):A10-A13, 2006
BASIC PRINCIPLES OF STRESS ECHO • ↑ Cardiac work load - ↑O2 demands- demand supply mismatch- ischemia • Impairment of myocardial thickening and endocardial motion
Treadmill vs supine bicycle advantage • Add information • Wide spread availability • Simple protocol • High work load • > Sensitive Disadvantage • Imaging post ex only Advantage • Image through out the exercise- peak • Onset of RWMA • Better image quality • Contrast stress echo • > Specific Disadvantage • Lower work load • Supine position affects ex.physio
Information obtained from Exercise Stress but not available with Pharmacological Test • Exercise Duration/Tolerance • Reproducibility of Symptoms with Activity • Heart rate response to exercise • Blood Pressure response • Detection of Stress Induced Arrhythmias • Assess control of angina with medical therapy • Prognosis
Indication pharmacological stress echocardiography • Inadequate exercise • Left bundle branch block • Paced ventricular rhythm • pre-excitation or conduction abnormality • Medication: beta-blocker, calcium channel blocker • Evaluation of patients very early after MI(<3 days) or • angioplasty stent(<2weeks) • Poor image degradation with exercise • Poor patient motivation to exercise
Pharmacologic Stress Agents Inotropic agents Dobutamine Arbutamine Coronary vasodilator Dipyridamole Adenosine Stress agents
DOBUTAMINE STRESS ECHO • Dobutamine- synthetic catecholamine • Inotropic & chronotropic- β1,β2 & α • Action: onset – 2 min half life – 2 min: continous IV • Metabolizd by cathechol-o-methyl transferase • Excretion: hepatobiliary system and kidney
Works by inducing myocardial ischemia • Modest ↑ SBP and ↓DBP • May be arrhythmogenic (0.7% rate in 8500 consecutive studies performed at Mayo Clinic) • Usually ineffective in patients on beta blockers • High rate of side effects • Hypotension induced does not have prognostic value unlike TMT • Does not interact with dipyridamole
Dipyridamole Potent coronary vasodilator Provoke anginal attack in angina patients Vasodilation effect inhibition of reuptake of adenosine by the endothelial cell CBF increases 4 to 5 times in normal vessel Reduction of subendocardial blood flow in stenotic coronary artery
Dipyridamole Coronary steal phenomenon Standard protocol: 0.54 mg/kg for 4 min High dose protocol: 0.84mg/kg Antidote: theophylline
Dipyridamole Contraindication active wheezing high degree AV block hypotension(SBP<90 mmHg) recent use of dipyridamole(<24 hours) Relative contraindication Hx of reactive airway disease sick sinus syndrome severe sinus bradycardia
Adenosine Naturally occuringagent Types of receptors A1: slowing HR and conduction A2a: c-AMP – decrease calcium uptake by SR -- smooth muscle relaxation vasodilation Half life: 2 seconds need constant IV infusion Rapidly removed from RBC and endothelial cell
Adenosine – side effect Flushng: 37% Dyspnea: 35% GI discomfort: 15% Headache:14% Light-headedness 9% Most side effect – short-lived and mild
Myocardial contrast in stress echo • Left vent opacification for border enhancement • Myocardial perfusion imaging • Perfusion at resting state-stress is performed and perfusion imaging is done at peak stress
Stress Echo Stress Echocardiography Diagnosis Prognosis Viability Treatment
Exercise –preferred-add information • > sensitive in CAD compared to dobutamine • Treadmill >sensitive, Bicycle>specific • Bicycle –during stress-> accurate presence and extend of disvs pat choice,availability etc. • Dobutamine is limited to pats who cant exert adequately & when the Q of viability is addressed • In pharmaclogical stress dobutamine is the agent- produces true ischemia than a flow mismatch
INTERPRETATION OF STRESS ECHO • Subjective assessment of regional wall motion • Compares wall thickening & endocardial excursion at baseline and stress • Limitation- subjective & nonquantitative • Measures like EF, ESV change, and strain rate to overcome limitations
Strain rate-myocardial velocity gradient -postsystolic shortening • TDI/Strain imaging> sensitive • Ischemia delays onset & rate of regional myo relaxation • Time quantified using TDI • QRS-onset of relaxation-350-400ms • Interval↓ by 34+/_10% in nl segments in response to high dose dopamine • ↓in interval is <12+/-18% in ischemic seg
Grade 1-normal 2-hypokinesis 3-akinesis 4-dyskinesis • Nl WMSI-1 at baseline and stress • Any score>1-abnormal • Good prognostic value
Hypokinesia-<5 mm of endocardial excursion • Akinesis - -vesyst thickening & endo excursion • Dyskinesis –systolic thinning & outward motion • nlresp-hyperkinesis • Absence –low work load, β blockade, cardiomyopathy & delayed post stress imaging • Localisation>specific in multivessel dis & in LAD than RCA/LCX
Prognostic value A new wall motion abnormality,rest & exercise WMSI,ESV response-correlated with risk
Prognostic value of stress echo • Independent predictors of cardiac events a)WMSI with exercise b) ST ↓≥1 mm c) treadmill time • Risk Index(RI)=1.02(WMSI)+1.04(ST change)− 0.14(Treadmilltime) • RI in upper quartile(+0.66 to+2.02)– risk was highest(30%) • Prognostic value is comparable in women and men
PRE-OPERATIVE RISK STRATIFICATION WITH DOBUTAMINE STRESS ECHO *Mayo Clinic, 530 Patients
Perioperative marker of coronary event • patients with a positive electrocardiographic response to treadmill stress test but no inducible wall motion abnormality on stress echocardiogram have a very low rate of adverse cardiovascular events during follow-up
VIABILITY OF MYOCARDIUM • That has the potential for functional recovery;- either stunned/hibernating myocardium • >6mm thickness -viable segment • Stunned or hibernating improved contractility with dobutamine , not in infarcted myocardium • Biphasic response – low dose ↑contractility(10 to 20 mcg/kg), at higher dose CBF ↓-- contractility ↓
Biphasic response is the most predictive of the functional recovery after revascularisation • Sustained improvement/no change-nonviable • For viability assessment – nuclear techniques are more sensitive dobut stress echo more specific PPV-similar NPV- favoursdobut stress echo