Download
1 / 52
520 likes | 732 Views
10 Questions must be answered i n Cardiac Surgical ICU. Question 1. Which factors must be checked when patients transferred from the operating room to the cardiac surgical ICU?. The patients is being well ventilated by: Observing chest movement Auscultating bilateral breath sounds.

E N D
10 Questions must be answered in Cardiac Surgical ICU Dr. Saffarian
Question 1 • Which factors must be checked when patients transferred from the operating room to the cardiac surgical ICU? Dr. Saffarian
The patients is being well ventilated by: • Observing chest movement • Auscultating bilateral breath sounds Dr. Saffarian
The ECG tracing demonstrates satisfactory rate and rhythm on the transport and then the bedside monitor. Dr. Saffarian
The blood pressure is adequate on the portable monitor and remains so after the arterial line is transduced and calibrated on the bedside monitor Dr. Saffarian
Question 2 • Which factors must be monitored in the ICU? Dr. Saffarian
1. ECG display and ECG 12-leads for detecting : • Rate • Rhythm • ST analysis Dr. Saffarian
2. Endotracheal tubes: • Confirmation of bilateral breath sounds and chest movement • Rechecking of the ventilator settings • Assessment of ABGs every 4hrs or after every major ventilator change • Very gentle suctioning of tracheal tube every few hours. Dr. Saffarian
3. Arterial lines for: • Monitoring of blood pressure • Obtaining of ABG Dr. Saffarian
Point Radial arterial line pressure measurements may not reflect the central aortic pressure when peripheral vasoconstriction is marked. In this situations, brachial or femoral arterial catheters provide more accurate measurement. Dr. Saffarian
Point Arterial lines should be connected to continuous heparin flushes to improve patency rates and minimize thrombus formation. Dr. Saffarian
Point Maintaining a radial arterial line for more than 3 days is associated with an increased risk of vessel thrombosis and line sepsis. Dr. Saffarian
Point Removal is indicated urgently if hand ischemia develops. Dr. Saffarian
4. Swan-Ganz pulmonary artery (PA) catheter: • Measuring LV filling pressure • Obtaining mixed venous oxygen saturation • Determining thermodilution cardiac output Dr. Saffarian
5. Central venous catheter (CVP): • Measuring RV filling pressure • Estimating of LV filling pressure in the absence of RV failure or mitral stenosis. • Determining of volume status Dr. Saffarian
6. Chest tube: • In mediastinum and into the pleural spaces if they are entered during surgery. • Drainage should be recorded hourly or more frequently if there is evidence of significant bleeding. • Chest tubes are connected to a drainage system o which 20 cm H2O suction is applied. Dr. Saffarian
Point Suctioning of clotted chest tubes with endotracheal suction catheters should be discouraged because it may introduce infection. Dr. Saffarian
Point When pleural tubes were placed, intrapleural pressure became equal to atmospheric pressure therefore pleural tubes must be removed in full inspiration because of minimal distance between viseral & pariental surface of pleura at this stage. Dr. Saffarian
Question 3 • Guideline for removal of lines and tubes in ICU. Dr. Saffarian
The Swan-Ganz catheter should be removed when inotropic support and vasodilators are no longer necessary. Dr. Saffarian
The CVP catheter should be removed when hemodynamic and volume status were stable. Dr. Saffarian
Arterial line should be removed after a stable postextubation blood gas has been obtained. Dr. Saffarian
The urinary catheter can be left in place if the patient is undergoing vigorous diuresis or has an increased risk of urinary retention. It should otherwise be removed once the patient is mobilized out of bed, usually on the second postoperative day. Dr. Saffarian
Chest tubes should be removed when the total drainage is < 100cc for 8hrs. Mediastinal tubes should always be removed off suction because graft avulsion has been know to occur if suction is maintained. Dr. Saffarian
A CXR is not essential after mediastinal tube removal but should be performed after removal of pleural chest tubes to rule out a pneumothorax. Dr. Saffarian
Question 4 • Etiology of mediastinal bleeding. Dr. Saffarian
1. Surgical bleeding: • Suture lines, soft tissues, sternum • Raw surface caused by previous surgery, pericarditis or radiation therapy. Dr. Saffarian
2. Anticoagulant effect: • Residual heparin effect • Quantitative platelet defects (heparin, quinidine, antibiotics, hemodilution, protamine) • Qualitative platelet defects ( ASA, uremia, CPB) • Depletion of coagulation factors • Fibrinolysis • Pre-existing coagulation abnormalities Dr. Saffarian
Question 5 • Preventilation of perioperative blood loss Dr. Saffarian
Warfarin should be stopped about 4 days before surgery to allow for resynthesis of Vit-K dependent clotting factors. ASA should be stopped 7 days before surgery. BT is usually normal with PLT counts as low as 70,000 and also in patients taking ASA. Dr. Saffarian
Heparin induced thrombocytopenia, may develop in patients receiving IV heparin for several days before surgery . Dr. Saffarian
Surgery should be delayed at least 24 hrs, in patients receiving thrombolytic therapy. Dr. Saffarian
Pre-operative dipyridamole 100mg qid leading to improved platelet function after CABG. Aprotinin is a serine protease inhibitor that prevent bleeding. It has been associated with an increased risk of graft thrombosis. Tranexamic acid is a potent inhibitor of plasminogen. Dr. Saffarian
Question 6 • Management of postoperative mediastinal bleeding. Dr. Saffarian
Ensure that chest tubes are patent Warm patient to normothermia Control hypertension and shivering PEEP in 2.5-5 cm H2O increments Check results of coagulation studies Dr. Saffarian
Protamine 25mg IV for two doses Desmopressin (DDAVP) 0.3 g/kg IV over 20 minute Packed cell if Hct< 28% PLT, 1 unit/10 kg Dr. Saffarian
FFP, 2-4 units Cryoprecipitate, 1 u/10kg Avoid hetastarch and 5% Albumin Epsilon-aminocaproic acid (EACA) if fibrinolysis is confi….. Dr. Saffarian
Question 7 • Diagnosis of cardiac tamponade Dr. Saffarian
Elevated central Venous pressure Decreased blood pressure Reflex tachycardia Shortness of breath Wide mediastinom Occasionally decreased mediastinal tube drainage Dr. Saffarian
Treatment of cardiac tamponade Volume expansion Control of mediastinal bleeding Pericardial drainage Dr. Saffarian
Question 8 • Post operative fever Dr. Saffarian
Fever is very common during the first 48-72 hrs and is usually caused by atelectasis from splinting and poor respiratory effect. Dr. Saffarian
Etiology of fever after the first 72 hrs Atelectasis or pnemonia Urinary tract infections Sternal or leg wound infections Post pericardiatomy syndrome Drug fever Catheter sepsis Endocarditis Intra abdominal process DVT or pulmonary emboli Dr. Saffarian
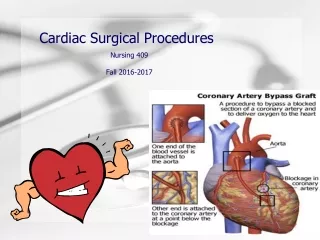
Question 9 • ECG changes after CABG Dr. Saffarian
These changes are nonspecific Convex ST elevation revealed pericardial irritation Concave ST elevations associated with significant rise of CPK-MB and traponins revealed postoperative MI Dr. Saffarian
New Q wave without rise of cardiac enzymes just revealed myocardial irritation or cardiac rotation. Nonspecific T wave changes are not important. Dr. Saffarian
New LBBB associated with rise of cardiac enzyme may be a sign of MI. Inflammation of bundle branch can lead to different types of bundle branch block Dr. Saffarian
Question 10 • Fluid administration in early post operation period Dr. Saffarian
Most patients return from the operating room about 5-10 kg above their pre-operative weight because of interaoperative fluid administration this represents a state of both total body sodium and water overload Dr. Saffarian
In general, DS/0.2% normal saline is given at a maintenance rate of 50cc/hr on arrival in the ICU to minimize an additional sodium load at a time when the kidneys have a tendency to retain sodium Dr. Saffarian