Download
1 / 41
410 likes | 517 Views
PRESCRIPTION DRUG ABUSE. Pharmacology: Drugs and Disease - Feb. 25, 2004. Greg Connell, Ph.D. Office: 3-126 BSBE; Phone: 624-3132 Email:gconnell@lenti.med.umn.edu. Drug Abuse. 1. Definitions. 2. Biological basis of drug abuse. 3. Prescription drugs with abuse potential.

E N D
PRESCRIPTION DRUG ABUSE Pharmacology: Drugs and Disease - Feb. 25, 2004 Greg Connell, Ph.D. Office: 3-126 BSBE; Phone: 624-3132 Email:gconnell@lenti.med.umn.edu
1. Definitions 2. Biological basis of drug abuse 3. Prescription drugs with abuse potential 4. Reasons to be aware of a potential for drug abuse 5. Individuals to be concerned about 6. Physicians who prescribe inappropriately 7. Protecting yourself from the professional patient Overview
1: Definitions A. Physical dependence • A normal physiological adaptation to repeated use of some categories of drugs • Examples may include: • down-regulation of receptor number • decreased efficiency of the coupling of the receptor to the • signal transduction mechanism • alteration of the drug’s metabolism
1: Definitions B. Tolerance • Occurs when increasing amounts of the drug are required to achieve the same physiological or psychological effect. • Indicative of the development of a physical dependence.
1: Definitions C. Cross-tolerance • The development of tolerance to one drug also increases tolerance to related drug categories
1: Definitions D. Withdrawal syndrome • Occurs when drug administration to a physically dependent • person is abruptly terminated • Symptoms are characteristic of the class of drug and tend to • be opposite the original effects of the drug before tolerance • developed
1: Definitions E. Psychic or psychological dependence • The individual believes that the presence of the drug is necessary to maintain a state of well being. • All major drugs of abuse produce a negative emotional state in dependent humans during acute abstinence. • Regaining a sense of well-being provides a positive • reinforcement or craving for continued abuse
1: Definitions F. Drug abuse • A behavioral definition: the self-administration of a drug for non-medical purposes resulting in either a psychic and/or physical dependence. G. Drug misuse • Results from either ill advised patterns of prescribing by • physicians or improper use by patients within the context of • medical treatment.
1: Definitions H. Addiction • A behavioral definition: recurrent drug use becomes the primary goal and disrupts the ability to function in family, social or career settings rather than being an incidental part of life. • Characterized by three major elements: 1. Compulsion to seek and take the drug 2. Loss of control in limiting intake 3. Emergence of a negative emotional state when access to the drug is prevented
2: Biological Basis of Drug Abuse A. An Evolutionary Perspective • The neural mechanisms that regulate emotion and behavior • were shaped by natural selection to maximize Darwinian • fitness. • “Love joins hate, aggression, fear expansiveness, withdrawal and so on, in blends designed not to promote the happiness of the individual, but to favor the maximum transmission of the controlling genes “ (E.O. Wilson)
An Evolutionary Perspective • Drugs of abuse are inherently pathogenic because they create a signal in the brain that indicates, falsely, the arrival of a huge fitness benefit and thereby hijack the incentive mechanisms of liking and wanting.
2: Biological Basis of Drug Abuse B. A Biochemical Perspective • The occasional use of an abusable drug is distinct from • repeated use and the emergence of chronic drug addiction. • The cellular and molecular mechanisms that mediate • the transition from occasional controlled drug use to addiction • are only just beginning to be understood.
Biochemistry of Drug Abuse • Drug use results in changes to specific neurotransmitter systems • within a highly limited band of structures including specific • parts of the amygdala and nucleus accumbens.
Biochemistry of Drug Abuse • Changes occur in the signals mediated by several • neurotransmitters including but not limited to dopamine, • opioid peptides and cotropin-releasing factor. • Increases in neurotransmitter concentrations can result in several short-term and long-term changes.
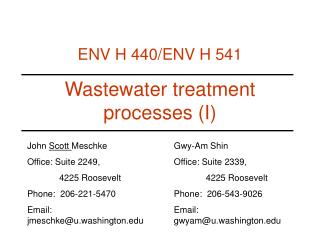
OH CH2CH2NH2 OH Biochemistry of Drug Abuse (dopamine) adenyl cyclase g B Gs ATP dopamine receptor GTP GDP cAMP cAMPdependent kinase alterations in gene expression cAMP response element- binding protein
Significance of Dopamine • Sex, chocolate, alcohol, marijuana, amphetamine, cocaine, • nicotine and heroin all directly or indirectly increase the • synaptic dopamine concentration within a highly localized • region of the brain. • Dopamine system plays a fundamental role in encouraging • behaviors, such as feeding, needed for life in organisms • ranging from slugs to primates.
Facilitated Learning Hypothesis • Dopamine release highlights or draws attention to certain • significant events and by underscoring such events the • dopamine signal helps the animal to learn to recognize them • and in some cases to repeat them.
3. Prescription Drugs with Abuse Potential • Drugs that produce a pleasurable effect such as an elevated mood, euphoria or calming. • Drugs that do not produce a mood altering effect are rarely • intentionally abused. • an exception is anabolic steroid use by athletes
3. Prescription Drugs with Abuse Potential Opioid agonists -heroin, morphine, meperidine, oxymorphone, hydrocodone, fentanyl, sufentanil i. abuse potential: (+++) high ii. acute intoxication: euphoria, rush sedation iii. withdrawal symptoms: (+++) high but are rarely life threatening. Symptoms can include opioid craving, irritability, hyperalgesia, cramps, muscle aches, nausea/vomiting, mydriasis, sweating, tachycardia, hypertension, fever.
Opioid Agonists additional consequences: (+++) high; life-expectancy decreased by 50%; i.v. users risk HIV infection. v. treatment • switch from short-acting drug to long-acting drug like • methadone • clonidine: a2 agonist reduces aspects of withdrawal • naltrexone
3. Prescription Drugs with Abuse Potential B. anxiolytic-sedative-hypnotics B.1: Barbituates: secobarbitol, pentobarbitol, amobarbitol abuse potential: (+++) high Acute intoxication: 1. Stimulant-like effects at low doses: euphoria, increased talkativeness 2. Depressant at high doses: ataxia, slurred speech
B.1: Barbituates Anxiolytic-Sedative-Hypnotics withdrawal symptoms: (+++) high; life threatening, tremor, nausea, sweating, hypertension, seizures iv. additional consequences: (+++) high; death from overdose, suicide B.2: Benzodiazepines: diazepam, flurazepam abuse potential: (+) low acute intoxication: similar to barbiturates withdrawal symptoms: (++) intermediate; cramps, agitation, anxiety, rarely seizures
CH 3 3. Prescription Drugs with Abuse Potential C: Stimulants C.1: amphetamine i. structure: CH NH CH 2 2 • amphetamine is a mixture of two stereoisomers: 1. d-isomer (dextroamphetamine) - stimulates the CNS more effectively than the l-isomer 2. l-isomer (levoamphetamine) - stimulates the cardiovasculature system more than the d-isomer
Amphetamine ii. function: • increases the synaptic dopamine concentration resulting • in an increased state of wakefulness and attentiveness. • acts primarily on two areas of brain: 1. reticular activating system (regulation of sensory input into the brain) 2. medial forebrain bundle (pleasure center)
Amphetamine iii. clinical uses: • narcolepsy • attention deficit hyperactivity disorder (ADHD) • appetite suppression -discouraged now because there is significant abuse potential iv. adverse effects: • cardiovascular side effects • irritability, nervousness, restlessness • long-term intoxication can result in a schizophrenia- like reaction
Amphetamine v. abuse potential: (++++++) very high acute intoxication: euphoria, increased alertness, increased motor activity vii. withdrawal symptoms: (+) low; drug craving, fatigue, bradycardia viii. additional consequences: (+++) high; depression, toxic-psychosis, cerebrovascular and cardiovascular accidents
Stimulants C.2 Methylphenydate (Ritalin) • Structure, clinical uses, adverse effects and withdrawal • symptoms similar to amphetamine. • Mild CNS stimulant that does not have significant peripheral actions. • Mechanism of action is not completely understood, but it may involve blockage of dopamine uptake.
3. Prescription Drugs with Abuse Potential D. Marijuana (D -tetrahydrocannibinol) i. therapeutic uses: Approved (THC) for the prevention of nausea and stimulation of appetite in cancer patients receiving chemotherapy and in patients with AIDS. 2. Other uses that are not approved include: reduction of the intraocular pressure in glaucoma, analgesic, muscle relaxant. ii. mechanism of action: agonist acting on the endogenous cannabinoid receptors
Marijuana iii. abuse potential: (+) low iv. acute intoxication: euphoria, heightened sensory perception, hallucinations and motor impairment at high doses v. withdrawal symptoms: (+) low; restlessness, irritability, agitation, sleep disturbances, nausea
4. Reasons to be Aware of a Drug Abuse Potential • A professional responsibility to prescribe drugs appropriately • The physical and mental condition of the patient is often related directly or indirectly to drug abuse • A personal responsibility not to become an easy target for • diversion
5. Individuals of Concern • The “professional patient” • Type I patient - obtains drugs of abuse through deception • of health care providers. • Type II patient - initially takes drugs for a legitimate • medical condition but later becomes addicted. • Health care professionals - potential for self-medication
6. Physicians Who Prescribe Inappropriately • Common causes for Minnesota Medical Practice actions: • prescribing for patients with known dependencies or addiction histories • prescribing controlled substances for chronic pain, anxiety or insomnia without proper reassessment. • prescribing without performing physical examinations. • prescribing in the face of known drug interactions.
6. Physicians Who Prescribe Inappropriately • “The Four “Ds” - Physicians as sources of drug diversion (AMA National Informal Steering Committee on Prescription Drug Abuse) • dishonest • disabled • deceived • dated
7. Protecting Yourself from the Type I Patient • Protection of prescription pads • store unused prescription pads in a safe place • minimize the number of pads in use at one time • have prescription blanks numbered consecutively so that missing sheets would be detected • never sign prescription blanks in advance • Write out the actual quantity in addition to using an Arabic or Roman numeral • Do not use prescription blanks for writing notes or memos
7. Protecting Yourself from the Type I Patient • Patient behavior which may suggest drug abuse • request for specific medications • request for higher or more frequent dosing • claims of allergy or lack of efficacy of specific drugs • evasive answers regarding medical history • traveling through town -not a resident • does not give name of primary or referring physician • claims to have lost prescription • requests appointment for late afternoon
LECTURE OBJECTIVES Understand the following definitions: • physical dependence • tolerance • cross-tolerance • withdrawal • psychic or psychological dependence • drug abuse • drug misuse • addiction 2. Be aware of the biological basis of addiction and the major classes of abused drugs: opioids, anxiolytic-sedative-hypnotics, stimulants, marijuana