Download
1 / 67
680 likes | 1.13k Views
Melanoma Overview 2009. Frances Collichio Associate Professor, University of North Carolina, Chapel Hill. What is Melanoma?. A Cancer of Melanocytes All Melanomas are malignant Melanocytes? Cells that Make Pigment Melanoma therefore can start from any pigmented cell. .

E N D
Melanoma Overview 2009 Frances Collichio Associate Professor, University of North Carolina, Chapel Hill
What is Melanoma? • A Cancer of Melanocytes • All Melanomas are malignant • Melanocytes? • Cells that Make Pigment • Melanoma therefore can start from any pigmented cell.
Extracutaneous Melanomas, • Mucosal • GI tract, Head and Neck, vagina • Older pts • Poorer px • Disporportionally non-white • Ocular • Ciliochoroidal • Poor prognosis • Iris • Better px
Unknown Primary • 2-4% of all melanoma • 9% of melanoma with lymph node involvement • Search for the primary • Ocular exam when there are liver mets When you cannot find the primary, treat these as if they started in the skin.
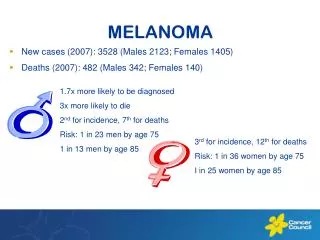
“Silent”NationalEpidemic • The incidence per year is rising faster than any other cancer! Rate/100,000 1:1500 1:600 1:250 1:150 1:135 1:75 1:65 1:60 estimated Lifetime Risk
2007 Estimated US Cancer Cases* Men766,860 Women678,060 • 26% Breast • 15% Lung & bronchus • 11% Colon & rectum • 6% Uterine corpus • 4% Non-Hodgkin lymphoma • 4% Melanoma of skin • 4% Thyroid • 3% Ovary • 3% Kidney • 3% Leukemia • 21% All Other Sites Prostate 29% Lung & bronchus 15% Colon & rectum 10% Urinary bladder 7% Non-Hodgkin 4% lymphoma Melanoma of skin 4% Kidney 4% Leukemia 3% Oral cavity 3% Pancreas 2% All Other Sites 19% *Excludes basal and squamous cell skin cancers and in situ carcinomas except urinary bladder. Source: American Cancer Society, 2007.
Melanoma US 2008 • 108,000 estimated new cases • 62,480 invasive • 48,290 in situ • 8,420 deaths www.cancer.org
Etiology • Inheritance -Chromosome 9 (10-40%) • Environment • Sun • Tanning Booths • Genes-Environment Interactions
Melanoma A—Asymmetry B—Border C—Color D—Diameter E—Evolution: A changing mole
Nodular Amelanotic Melanoma Invasive Melanoma
After diagnosing a skin lesion as melanoma, what is next? • Surgery on the primary by an experience surgeon or dermatologist • The margins of resection around the primary depend on the depth of the primary • Less than 1mm deep, 1cm margin • 1 to 2mm deep, a 1 to 2cm margin • Greater than 2 mm deep, a 2 cm margin
Staging, 2002 AJCC • T • Breslow depth • Clark level---used only in T1 melanomas • Ulceration • N • N1 one node is involved • N2 one to three • N3 4 or more, matted nodes, in transit disease, or satellites (tumor w/in 5cm of the primary). • Micro or Macro in all three cases • M • M1a-skin, subcutaneous tissue or distant lymph nodes • M1b-lung • M1c-other sites
Example • Stage IIB • T is 4mm without ulceration • Or T is 2 to 4 mm with ulceration • No nodes are involved. • No mets • Patients often think that 4mm tumor is not stage 4
Sentinel Lymph Node Evaluation Lymph node serially sectioned while fresh Alternate sections paraffin-embedded; remainder snap frozen MS01-1234 Level 1 S-100 Doe, John MS01-1234 Level 2 H&E Doe, John MS01-1234 Level 3 H&E Doe, John MS01-1234 Level 4 H&E Doe, John MS01-1234 Level 5 H&E Doe, John MS01-1234 Level 6 H&E Doe, John MS01-1234 Level 7 S-100 Doe, John Five H&E-stained sections flanked by two S-100 sections
Morton, NEJM 2006 • Nodal relapse in the observation 15.6% • Nodal relapse in the treated group 3.4% • 5 year survival 72.3% for patients with sentinel node involvement treated with immediate lymphadenectomy vs 52.4% for those with recurrent disease
Morton, NEJM 2006 • Sentinel lymph node biopsy identifies patients who would otherwise require lymph node surgery at relapse • The earlier initiation of complete lymph node dissection may improve overall survival • Accurately predicts prognosis
Indications for the Sentinel Lymph Node Procedure • Thin melanomas (< 1 mm) • Risk: 5% (Annals of Surgical Oncology Oct 2004) • UNC: balanced discussion 0.5-1.0 mm • Intermediate thickness melanomas (1-4 mm) • Risk: 18-20% • UNC: All patients (NEJM 2006) • Thick melanomas (>4 mm) • Risk: 40%+ nodal, 15-20% systemic • UNC: All patients
Patients with Postive Lymph Nodes • Have completion Lymph node surgery.
After treating the primary and completing lymph node surgery, what is next?
Now • You know the T stage • You know the N stage • You base the extent of additional studies on those two facts.
Additional Studies? • Stage I to IIA: (up to a 4mm thick with no ulceration) No additional Studies • Stage IIB, IIC: Additional Studies as clinically indicated • Stage III: Baseline studies for staging or symptoms---Chest x-ray, CT + PET, MRI brain
Why PET/CT • CT commonly used alone • Can miss visceral/lung metastases Reinhardt, MJ et al. J Clin Oncol 2006;24:1178
Treatment of Stage III Melanoma when all of the visible tumor has been removed • Observation • Clinical Trial • Or Interferon alpha
Treatment of Stage III Melanoma • Only one FDA Approved Therapy • Interferon-a 2b (Brand Name: Intron) • Meta-Analysis ~ 10% Absolute Benefit in RFS • Improved QoL versus Observation • Cost Effective • Patient Preference compared to increased risk • 3% survival benefit Cole, BF et al. J Clin Oncol 1996;14:2666 Hillner, BE et al. J Clin Oncol 1997;15:2351 Killbridge, KL et al. J Clin Oncol 2001;19:812
Adjuvant Radiation Therapy • Consider RT to the nodal basin when there are multiple nodes involved or extranodal extension (category IIb evidence NCCN)
Treatment of Stage III melanoma that cannot be surgically removed • In transit disease • Matted Lymph nodes • Clinical trials • Local infusions of chemotherapy or immune therapy • Radiation • Chemotherapy
Management of Stage IV • Median survival is 9 months and less than 5% probability of survival beyond 5 years. • Surgery • Best for skin/lymph nodes>lung>GI tract • Radiation • Palliation of symptomatic sites • High dose fractions (?) • Brain Mets
“Standard Systemic Treatments” • Clinical Trial • Small Molecule Targets • Immune modulating agents • High-dose IL-2 • Vaccines • Chemotherapy • DTIC or temozolamide • Paclitaxel with or without platinum • New agents
Immune Modulating AgentsHigh Dose IL 2 • Increases CD 4 positive cells • Pooled analysis ORR 14% • CR 5% • Highly selected patients • Most durable response of the known therapies • Toxic. Requires ICU care and expert personnel
Any hope for Vaccines ? • Stage IIIB and IV • OncoVEXGM-CSF will be administered by injection into all injectable cutaneous, subcutaneous or nodal lesions lesions, every two weeks. • This vaccine uses Herpes virus proteins as a co-stimulant
Resolution of un-injected disease in the lung. Injection sites in the knee/thigh
CTLA -4 Blockade: Clinical Development • Fully human monoclonal antibodies • Ipilimumab (MDX-010)—IgG • Ticilimumab (CP-675,206)--IgG
Durable Complete Response in Metastatic Melanoma • Complete resolution of 2 subcutaneous nodules, 31 lung metastases and 0.5 cm brain metastasis. Patient previously failed chemotherapy and surgery. • Response ongoing at 40+ months Sources: Phan et al. PNAS. 2003 Jul;100(14):8372-8377 and Medarex unpublished data Duration as of 1/10/05.
Our Case • 53 year old • Resection • of brain melanomas 4/2005 • in the small intestine 9/2005 • under the skin 11/2005 • Six months of temodar • Disease free for one year • CTLA 4 inhibitor • Recurrence in the skin, lung and bone summer 2007 • Severe joint pain and decrease in performance status. • Prednisone • After initial increase in skin mets, he went into a complete remission and has been in remission for over a year