Download
1 / 26
280 likes | 669 Views
The Alcohols. By S. Bohlooli, Ph.D. History. The alcohol had important place in humankind for at least 8000 years The diluted alcoholic beverages were preferred over water, In western countries Today, 75% of US adult population drinks alcohol regularly

E N D
The Alcohols By S. Bohlooli, Ph.D
History • The alcohol had important place in humankind for at least 8000 years • The diluted alcoholic beverages were preferred over water, In western countries • Today, 75% of US adult population drinks alcohol regularly • About 10% of the general population in the US are alcohol abuser.
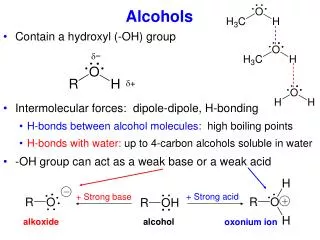
Basic Pharmacology ofEthanol • Pharmacokinetics • Ethanol is a small water soluble molecule • Presence of food delays absorption • Vd approximates total body water • Over 90% of alcohol consumed is oxidized in the liver. • Rate of oxidation follows zero order kinetics.
Metabolism of ethanol • Alcohol Dehydrogenase pathway • Microsomal ethanol oxidizing system (MEOS). • Acetaldehyde metabolism
Ethanol CH3CH2OH NADPH + O2 NAD+ MEOS Alcohol Dehydrogenase (ADH) Θ NADH Acetaldehyde CH3CHO NADP+ Disulfiram NAD+ Θ Fomepizole Aldehyde Dehydrogenase NADH Acetate CH3COO- Alcohol Dehydrogenase (ADH) pathway
Microsomal Ethanol Oxidizing System (MEOS) • At concentration below 100 mg/dl the MEOS has little contribution to the ethanol metabolism. • During chronic consumption there is an induction in enzyme activity • Enzyme inducing drugs like phenobarbital may increase activity of MEOS.
Acetaldehyde metabolism • It seems several enzymes are responsible for acetaldehyde metabolism • The primary enzyme system is aldehyde dehydrogenase • The product is acetate • Oxidation of acetaldehyde is inhibited by disulfiram. • Co-cosumption of ethanol and disulfiram leads to acetaldeyde accumulation. • Facial flushing, nausea, dizziness and headache are the main unpleasant reaction.
Pharmacodynamics of acute ethanol consumption • Central nervous system • Sedation, relief of anxiety, • Slurred speech, impaired judgment, disinhibited behavior • Condition called “intoxication” or “drunkenness” • There is too different between tolerant and nontolerant individuals • At higher blood concentration: • Coma, respiratory depression and death.
Ethanol Mechanism of action • Enhances the action of GABA at GABAA • Inhibits the action of Glutamate at NMDA • Disruption of biological membranes through reduction in lipid viscosity (fluidization)
Effect on Heart • Depression of myocardial contractility (blood concentration > 100 mg/dl) • It seems that acetaldehyde is responsible for ultra structural changes
Effect on Smooth Muscle • Vasodilator • Depression of vasomotor center • Direct effect • Relaxes Uterus
Consequences of Chronic Alcohol Consumption • Liver and gastrointestinal tract • Nervous system • Tolerance and physical dependence • Neurotoxicity • Cardiovascular system • Blood • Endocrine system and electrolyte balance • Fetal alcohol syndrome • Immune system • Increased risk of cancer
Liver and gastrointestinal tract • About 15-30% chronic heavy drinkers develop sever liver disease: • Alcoholic fatty liver • Alcoholic hepatitis • Cirrhosis and liver failure • Increased ratio of NADH/NAD+reduced gluconeogenesis, hypoglycemiaa nd ketoacidosis • Excess of Acetaldehyde (very reactive compound) • Decreased level of Glutathione • Hormonal factors • Increased gastric and pancreatic secretion. • Altered mucosal barriers • Malabsorption of water soluble vitamines
Nervous system • Tolerance and physical dependence • Metabolic tolerant • Neurotransmitters, receptors, ion channels, enzymes that participate in signal transduction pathway • Acute increase in local concentration of serotonin, opioids, and dopamine • Withdrawal syndrome • Hyperexcitability, convulsion, toxic psychosis • Dose, rate and duration of alcohol consumption
Nervous system • Neurotoxicity • Generalized symmetric peripheral nerve injury • Gait disturbance and ataxia • Wernicke-Korsakoff syndrome • Thiamine deficiency • Impaired visual acuity
Cardiovascular system • Heavy alcohol consumption dilated cardiomyopathy • Depressed function of mitochondria and sarcoplasmic reticulum, intracellular accumulation of fatty acids and phospholipids up regulation of voltage dependent calcium channels. • Arrhythmias • Arrhythmias Seizure, syncope and sudden death during alcohol withdrawal • Hypertension • Low coronary heart disease high HDL
Blood • Mild anemia alcohol related folic acid deficiency • Hemolytic syndromes • Abnormalities in platelets and leukocytes
Endocrine system and electrolyte balance • Gynecomastia and testicular atrophy • Alcoholic with chronic liver diseases ascites, edema and effusions. • Low potassium • Hypoglycemia, ketosis
Fetal alcohol syndrome • Heavy drinking in first trimester • Retard body growth • Microcephaly • Poor coordination • Underdevelopment of mild facial region
Immune system • Alteration in: • Chemotaxis of Granulocytes • Lymphocyte response to mitogens • T cell numbers • Natural killer cell activity • Level of tumor necrosis factor
Increased risk of cancer • Increased risk for cancer of: • The mouth, pharynx, larynx, esophagus and liver • Breast • Alcoholic beverages may carry potential carcinogens
Alcohol – Drug interactions • Pharmacokinetics • Chronic intake: • Alcohol induced increase drug metabolism • Increased level of Acetaminophen toxicity • Acute intake: • Drug metabolism inhibition • Pharmacodynamics • Additive central nervous system depression
Management of acute alcohol intoxication • Degree of intoxication depends on: • The blood ethanol concentration • The rapidity of the rise of the alcohol level • The time during which the blood level maintained.
Management of alcohol withdrawal syndrome • The major objective of drug therapy is prevention of: • Seizure • Delirium • Arrhythmias • Potassium, magnesium and phosphate balance • Thiamine therapy • Replacement therapy with long acting sedative-hypnotic drugs
Pharmacotherapy of alcoholism • Disulfiram • slow elimination rate • Inhibitor of other drug’s metabolism (phenytion, isoniazide) • Compliance is low • Some drugs have Disulfiram like effect : metronidazole, sulfonylurea hypoglycemic drugs • Naltrexone • Decreased rate of relapse • Reduced alcohol craving • Acamprosate • Weak NMDA receptor antagonist • GABAA Activator • Reduce replapse
Pharmacology of other alcohols • Methanol • Ethylene Glycol • Drug therapy: ethanol, fomepizole