Download
1 / 62
630 likes | 775 Views
How to Examine the Heart and Blood Vessels. Joel Niznick MD FRCPC. Look at the patient. Sick/well Comfortable/in distress Cyanosed/plethoric Wet/dry Young/old Male/Female Establish probabilities of disease History will have told you what to suspect. Younger people

E N D
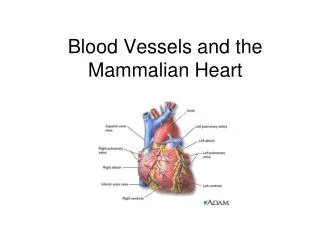
How to Examine the Heartand Blood Vessels Joel Niznick MD FRCPC
Look at the patient • Sick/well • Comfortable/in distress • Cyanosed/plethoric • Wet/dry • Young/old • Male/Female • Establish probabilities of disease • History will have told you what to suspect
Younger people Functional murmur vs MVP vs bicuspid AV Older people Aortic sclerosis vs aortic stenosis Common Clinical Scenarios
Males more commonly have aortic valve disease Young – BAV Elderly - Degenerative Females more commonly have mitral valve disease MVP > rheumatic heart disease Probabilities
Inspect • Facies/body habitus • Cyanosis • Xanthelasma • Arcus senilis • Conjunctival hemorrhages • Syndromes • Marfan’s • Down’s
Hands • Clubbing • Capillary return • Digital ischaemia • Splinter hemorrhages • Osler’s nodes • Janeway lesions
Blood pressure • At rest 5” • Both arms • Legs if young hypertensive
Look at the Fundi OSU Interactive Physical Exam Guide
Look at the Fundi • Disc • Vessel • Hemorrhages • Exudates
Pulses • Rate • Rhythm • Volume • Quincke’s • Water hammer • Brachio-radial delay
Carotid • Upstroke-normal/brisk/delayed/anacrotic • Volume-normal/increased/decreased • Auscultate: • Bruit • Murmur • S2 audible ? Over carotid?
JVP • Height • Waveform • Specific patterns • Response to maneuvers • Inspiration • HJR
JVP Summary • Confirm it’s the JVP you are seeing • Compressibility • Waveform • Manoeuvers • Identify the height – start at 30o • Identify the waveform
If unable to see JVP-lie patient flat If still unable to see JVP-sit patient upright
Normal JVP Waveform a c v x y x
JVP Inspection • Look for descents not waves • Descents are easier to see due to greater amplitude and frequency • Time deepest descent with systole. This is the X’ descent
Precordium • Palpate: Aortic → Pulmonary → LSB → Apex → Left decubitus • Thrills • Palpable HS • Lifts • Apex: size/position/motion
Auscultation • Follow same sequence • Aortic → Pulmonary → LSB → Apex → Left decubitus → Upright lening forward • Diaphragm except for apex (use both here) • Identify HS, then extra sounds, them murmurs • Dynamic maneuvers
Palpation - Precordium Parasternal: • Palpable P2-pulmonary HTN • Thrill • VSD/HCM • RV lift • RVH • Severe MR
Palpation - Apex Apex: • Palpable in 1 of 5 adults age 40 • Best felt with fingertips or finger pads Normal Location: • No more than 10 cm from mid-sternal line in the supine position • Left decubitus position not reliable for apical location Normal Size: • No larger than 3 cm (about 2 finger breadths)
Apex–Dynamic Abnormalities Sustained Apex: • correlates with pressure overload or LVF • ( > 2/3 systole-hangs out to S2) • AS, LVH or LV systolic dysfunction Hyperdynamic Apex: • correlates with volume overload AR/MR • palpable S4 (atrial kick) • palpable S1 (MS) • palpable non-ejection click (MVP)
Apex–Dynamic Abnormalities Atrial kick: • Palpable S4 • Loss of LV compliance • LVH 2o Hypertension • Aortic Stenosis • Hypertrophic Cardiomyopathy
Common Murmurs Systolic Murmurs • Aortic stenosis • Mitral insufficiency • Mitral valve prolapse • Tricuspid insufficiency Diastolic Murmurs • Aortic insufficiency • Mitral stenosis S1 S2 S1
Auscultation Grading of Murmurs: Grade 1 - only a staff man can hear Grade 2 - audible to a resident Grade 3 - audible to a medical student Grade 4 - associated with a thrill or palpable heart sound Grade 5 - audible with the stethoscope partially off the chest Grade 6 - audible at the bed-side
Characteristics of a “functional” murmur • Short and soft SEM • Normal S1 and S2 • Normal cardiac impulse • No evidence for any hemodynamic abnormality
Functional (Innocent) MurmursCommon in asymptomatic adults • Characterized by • Grade I – II @ LSB • Systolic ejection pattern - no with Valsalva/ upright • Normal precordium, apex, S1 • Normal intensity & splitting of second sound (S2) • No other abnormal sounds or murmurs • No evidence of LVH S1 S2
Characteristic of the NOT Innocent Murmur • Diastolic murmur • Loud murmur - grade IV or above • Regurgitant murmur • Murmurs associated with a click • Murmurs associated with other signs or symptoms e.g. cyanosis • Abnormal 2nd heart sound – fixed split, paradoxical split or single
Integrating Pulse with HS and Murmurs www.blaufuss.org
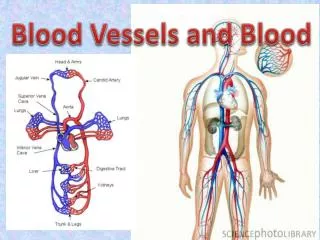
Retinal Carotids Brachial Renal Ulnar Radial Femoral Popliteal Posterior Tibial Dorsal Pedis
Examination of Pulses • Grading: • Normal/Increased/Decreased/Absent • 2+/3+/1+/0 • Allen’s test • Trophic changes/Ulceration • Perfusion • Pallor on elevation • Rubor on dependency • Venous refill with dependency (should be less than 30 seconds) • Bruits
Trophic Changes Shiny, hairless skin, dystrophic nail changes and dependent rubor associated with peripheral arterialocclusive disease of the patient's right foot
Pallor on elevation Rubor on dependency