Download
1 / 35
350 likes | 447 Views
Death, Taxes, and Rising Health Care Costs. Robert E. Hurley, Ph.D. Virginia Commonwealth University. Session Overview. Cost pressures The move to managed care Early success; later decline Consequences for States Private sector responses Tasks before you.

E N D
Death, Taxes, and Rising Health Care Costs Robert E. Hurley, Ph.D. Virginia Commonwealth University
Session Overview • Cost pressures • The move to managed care • Early success; later decline • Consequences for States • Private sector responses • Tasks before you
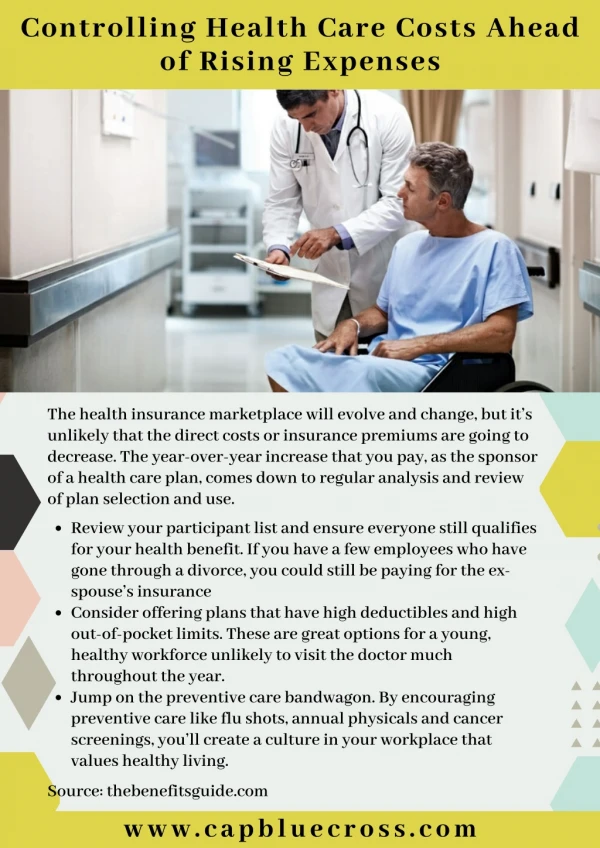
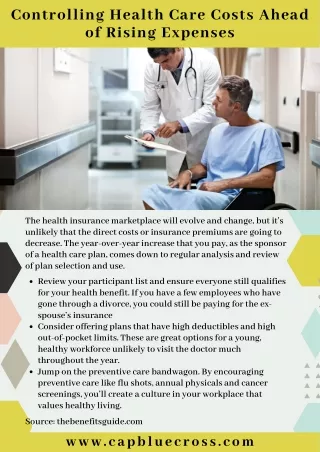
The Elusive Pursuit of Sustainable, Affordable Health Care Coverage • Purchasers of health benefits have long struggled to expand coverage, promote access, and contain costs—simultaneously • Public policymakers have assisted efforts with a variety of policy interventions to try to affect health care markets • States have pursued many strategies: certificate of need, rate regulation, investment in safety net providers, reform of insurance markets, mandated benefits and services, expanded public coverage, consumer protection initiatives • Cost containment, in particular, has proven to be elusive
Annual Change in Private Health Spending per Capita (Adjusted for Inflation), 1961-2001 9.1 Medicare and Medicaid Implemented Wage and Price Controls Managed Care and Threat of Health Reform Voluntary Effort Altman and Levitt, 2002
The U.S. Health System ― A Simplified View Government Employer 80 mil. 170 mil. • Aged (>65) • Disabled • Low income • Employee • Dependents Insurance carrier/Health plan/TPA Direct Purchase Direct Purchase Health Care Providers Uninsured = 45 mil.
Employer/Sponsored Indemnity Coverage A system built around spending someone else’s money . . .and an unmanaged system, at that Employer sponsorship―subsidized premiums and limited cost sharing, health benefits as non-cash compensation shielded from income tax Indemnity―freedom of choice of providers, providers fees not negotiated, little/no medical management, varied benefit packages
National employee enrollment by type of plan . Percent of All Covered Employees Gabel et al, KFF, 2002
Increases in Health Insurance Premiums Compared to Other Indicators, 1988 18% 12.7% 8.5% 8.3% 4.8% 3.4% 1.6% 5.1% 4.1% Gabel et al, KFF, 2002
Percent of Premium Paid by Covered Workers Gabel et al, 2004
The Purchaser Revolution The employers make their move
Purchasers Attempt To Promote Competition via Managed Care • Private purchasers embraced managed care to exert more control over health benefits and costs • Managed care organizations (MCOs) charged with being aggressive purchasing agents • MCOs design/develop products to match purchaser (and consumer) demands with provider capacity and capabilities • Products to promote competitive dynamics to curb cost growth/improve efficiency/reduce cost shifting
From Indemnity to Managed Care Indemnity—freedom of choice of providers, providers fees not negotiated, little/no medical management, varied benefit packages Managed care—network-based delivery systems, negotiated payments, medical management, typically richer benefits • HMO—narrower networks, aggressive medical management, some risk-based payment • PPO—broader networks, limited medical management, discounted prices payment • POS—HMO with out-of-network options (“leaky HMO”)
National employee enrollment by type of plan . Percent of All Covered Employees Gabel et al, KFF, 2002
Increases in Health Insurance Premiums Compared to Other Indicators, 1988-1999 18% 12.7% 8.5% 8.3% 4.8% 3.4% .8% 1.6% Gabel et al, KFF, 2002
State Governments In 1990s Hitched Their Wagons to Managed Care and Market-based Models • State employee health benefits programs came to rely extensively on managed care products • By 2000, more than half (56%) of Medicaid beneficiaries enrolled in managed care arrangements • Many States enrolled SCHIP eligible children in managed care plans • Sustainability of coverage expansions conditioned on expectation of controlling cost increases • States promoted coverage and benefit expansions with various mandates on health plans
Bringing on a Counterrevolution • Suppression of cost-shifting • Consumer and provider backlash • “Uncontrollable cost pressures” • Declining public payments
The Decline of Cost-Shifting—1990-2000(payments received as a % of actual costs) 127% 89% 80% 112% 100% 96% MedPAC, 2002
Median U.S. Physician Income, 1988-1998 (in thousands) $ Modern Healthcare, 2001
Percent of Groups with “Unfavorable” Rating(Kaiser Family Foundation, National Survey of Prescription Drugs, Sept. 2000)
Percent Increase in Rx Spending vs. Total Health Care Spending, 1990-2002 Percent Source: HCFA/CMS
Medicare Makes Its Move—BBA* of 1997Percent Annual Increase in National Health Expenditures (NHE) vs. Private insurance and Medicare *Balanced Budget Act Modern Healthcare, 2001
Increases in Health Insurance Premiums Compared to Other Indicators, 1988-2004 18% 13.9% 11.2% 8.5% 8.3% 4.8% 2.3% 2.2% .8% Gabel et al, KFF, 2004
Contemporary Picture • Premium increases remain near or at double digits • Private coverage likely to continue to decline • Private-sector managed care plans lose traction in cost control efforts with providers • Continued increases in major cost drivers: labor, technology, pharmacy, malpractice, and administrative cost • Public payers continue to shift more pressure to private payers • Increased consumer cost participation inevitable
Managed Care—Managing to Hold On • Broader networks/looser products (PPO) • Targeted disease management programs to focus on high-cost users • Incentive-based compensation systems for providers to promote quality • Expanded consumer cost sharing and consumer engagement in choices • Raising premiums faster than costs
National employee enrollment by type of plan . Percent of All Covered Employees Gabel et al, KFF, 2002
Implications for State Policymakers Sharply rising health care expenses affect: • State employee benefits costs • Medicaid and SCHIP expenditures • Coverage expansions—past and future • Financing for safety net providers • Sustainability of private coverage—potentially increasing enrollment in public programs • Demands for both deregulation and new regulation
Medicaid—The Land Where Managed Care Succeeded, So Far • Managed care in Medicaid has fared better than in commercial sector because it is grounded in assumption that resources are limited • States have stayed with HMO product in part because substantial cost-shifting to consumer not an option • Most (but not all) States generally satisfied with prepaid health plans and ability to hold them accountable for cost and quality standards • Medicaid managed care emerging as lucrative industry for specialized plans; new opportunities to place greater demands on plans
The Private Sector Response • Disenchanted with managed care organizations, growing doubts about their ability to affect health care markets • Belief that expanded coverage/benefits with reduced out of pocket costs for employee/consumer is THE problem and needs to be reversed • Drumbeat building for a variety of “consumer directed health product” (CDHP) designs • Is this inspiration or desperation?
Percentage of Large Employers (>200 workers) Planning Selected Benefit Changes in Next Year Gabel et al, KFF, 2004 Likely= Very/Somewhat likely; Not=Other
Consumer Directed Products (CDHP)— A Continuum Perspective No premium contribution and “first dollar” coverage Premium contributions and cost sharing Sharply increased out-of-pocket costs/benefits buy-down High-deductible plan option with health savings/reimbursement accounts Defined contribution plans Cash in lieu of benefits
CDHP: Managed Care Under New Management Routine/ Discretionary Care EMPLOYEE’S Spending Account $ EMPLOYER $ High- Cost Care High Deductible Insurance Policy
Policy Concerns with Consumer Directed Products • Information to support consumers remains badly underdeveloped • Potential to lose group-based negotiating clout • Deferred/forgone care could lead to higher costs • Uncompensated care could rise sharply • Healthy likely to opt out of conventional insurance • Less healthy try to maintain comprehensive coverage • Risk-pooling undermined; premiums could soar • Fewer of the less healthy can afford coverage—become uninsured
The Tasks Before You • Sustain past coverage expansions and explore new configurations of public and private arrangements • Review strategies for purchasing care for Medicaid and SCHIP beneficiaries • Revisit benefit designs and delivery system options for State employees • Re-appraise regulatory and other interventions to bolster private insurance markets • Consider consequences of consumer directed products
Annual Change in Private Health Spending per Capita (adjusted for inflation), 1961-2001 Medicare and Medicaid Implemented Managed Care and Threat of Health Reform What Next? Wage and Price Controls Voluntary Effort Altman and Levitt, 2002
“You can always count on the Americans to do the right thing, after exhausting all other alternatives.” Winston S. Churchill