Download
1 / 38
380 likes | 606 Views
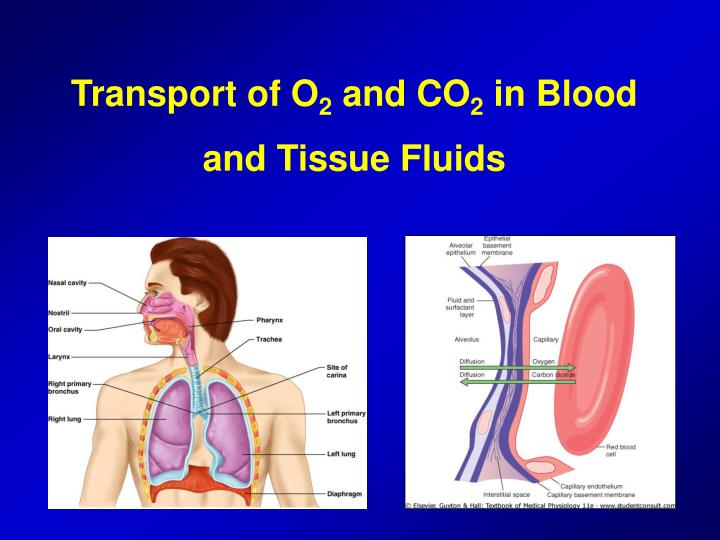
Transport of O 2 and CO 2 in Blood and Tissue Fluids. Transport of O 2 from the Lungs to Tissues. Uptake of O 2 by pulmonary capillary blood. Uptake of O2 by the pulmonary blood during exercise. Transport of O 2 in the Arterial Blood.

E N D
Uptake of O2 by pulmonary capillary blood • Uptake of O2 by the pulmonary blood during exercise
Transport of O2 in the Arterial Blood • About 98% of the blood that enters the left atrium has become oxygenated up to a PO2 of about 104 mmHg • On leaving the lungs, the PO2 of shunt blood is about that of normal systemic venous blood (40 mmHg) • Venous admixture of blood and new PO2 of about 95 mmHg in the pulmonary vein
Diffusion of O2 in from the peripheral capillaries into the tissue fluid • Whe the arterial blood reaches the peripheral tissues, its PO2 in the capillaries is still 95 mmHg • PO2 in the interstitial fluid that surrounds the tissue cells averages only about 40 mmHg
Effect of Blood Flow and O2 Consumption • Effect of rate of blood flow • Effect of rate of metabolism on interstitial PO2 • Tissue PO2 is determined by a balance between 1) the rate of O2 transport to the tissues in blood and 2) the rate at which the O2 is used by the tissues
Diffusion of CO2 from the Peripheral Tissue Cells into the Capillaries • At each point in the gas transport chain, CO2 diffuses in the direction exactly opposite to the diffusion of O2 • CO2 can diffuse about 20 times as rapidly as oxygen • Only 1 mmHg difference between venous and interstitial CO2 • CO2 pressures are approximately the following:
Effect of Rate of Tissue Metabolism and Tissue Blood Flow on Interstitial CO2
Role of Hemoglobin in O2 Transport • Normally about 97 % of O2 transported from the lungs to the tissues is carried in chemical combination with hemoglobin in RBC • The remaining 3% is transported in the dissolved state in the water of plasma and blood cells • Reversible combination of O2 with hemoglobin • When PO2 is high in the pulmonary capillaries, O2 binds with hemoglobin, but when PO2 is low as in tissue capillaries, O2 is released from the hemoglobin
Oxygen Transport: Role of Hemoglobin • Each hemoglobin molecule binds four oxygen atoms in a rapid and reversible process • The hemoglobin-oxygen combination is called oxyhemoglobin (HbO2) • Hemoglobin that has released oxygen is called reduced hemoglobin (HHb) Lungs HHb + O2 HbO2 + H+ Tissues
O2 - Hemoglobin Dissociation Curve • Saturation of arterial blood hemoglobin (95 %) • And saturation of hemoglobin 75 % when PO2 is about 40 mmHg in venous blood
Maximum amount of O2 that can combine with hemoglobin of blood • 15-16 gr hemoglobin / 100 ml blood • 1 gr hemoglobin can bind 1.34 ml of O2 • 15 x 1.34 = 20.1 ml O2
Transport of O2 during strenous exercise • In heavy exercise, muscle interstitial PO2 can decrease from 40 mmHg to as low as 15 mmHg • At this low pressure, only 4.4. ml of O2 remain bound with hemoglobin in each 100 ml of blood • Thus, 3 times as much O2 as normal is delivered • Utilization Co-efficient: Percentage of blood that gives up its O2 as it passes through the tissue capillaries • Normal value is about 25 % • During heavy exercise UC can increase to 75 %
Effect of Hemoglobin to “Buffer” the Tissue O2 • Tissue oxygen buffer system: hemoglobin in the blood is mainly responsible for stabilizing the tissue O2 pressue • Role of hemoglobin in maintaining nearly constant PO2 in the tissues: • At rest, the tissues require about 5 ml O2 / 100 ml blood • The tissue PO2 cannot rise above 40 mmHg, if it did, the amount of O2 needed by the tissues would not be released from hemoglobin • Hemoglobin sets the upper limit of O2 pressure at about 40 mmHg
Effect of Hemoglobin to “Buffer” the Tissue O2 • When atmospheric O2 concentration changes markedly, buffer effect of hemoglobin maintains constant tissue PO2 • When alveolar PO2 is decreased as low as 60 mmHg • When alveolar PO2 rises as high as 500 mmHg
Factors that shift the O2-Hemoglobin dissociation curve • Increased CO2 concentration • Increased blood temperature • Increased 2,3-biphosphoglycerate (BPG)
Bohr Effect: • Increased delivery of O2 to the tissues when CO2 is high • CO2 diffuses from the tissue cells into the blood • This increases blood PO2 which in turn raises blood H2CO3 and H ion concentration • Increased pH shifts the O2-hemoglobin dissociation curve to the right
Metabolic Use of O2 by the Cells • Effect of intracellular PO2 on rate of O2 uptake • Only a small level of O2 pressure is required in the cells for normal intracellular chemical reactions to take place • When the cellular PO2 is more than 1 mmHg, O2 availability is no longer a limiting factor • The main limiting factor is the concentration of ADP • The rate of O2 usage changes in proportion to the change in ADP concentration
Metabolic Use of O2 by the Cells • Effect of diffusion distance from the capillary to the cell on oxygen use: • Tissue cells are seldom more than 50 mm away from a capillary • Effect of blood flow on metabolic use of O2 • Transport of O2 in the dissolved state: • Only about 0.17 ml O2 is normally transported in the dissolved state to the tissues by each 100 ml blood • This constitutes only about 3% compared to 97% Hemoglobin
Combination of Hemoglobin with CO • Displacement of oxygen • Carbon monoxide combines with hemoglobin at the same point on the hemoglobin molecule as does O2 • CO can bind with about 250 times as much tenacity as O2 • A CO pressure of about 0.4 mmHg in the alveoli can equally compete with O2 to bind hemoglobin • It causes half the hemoglobin in the blood to become bound with CO instead of O2 • Even though O2 content of blood is reduced, PO2 of the blood may be normal
Transport of Carbon Dioxide in the Blood • CO2 can usually be transported in far greater quantities than oxygen can be • Under resting conditions, an average of 4 ml of CO2 is transported from the tissues to the lungs per 100 ml blood
Transport of CO2 in dissolved state • Amount of CO2 dissolved in the fluid of the blood at 45 mmHg is about 2.7 ml/dl • Amount dissolved at 40 mmHg is about 2.4 ml
Transport of CO2 in the form of bicarbonate • Dissolved CO2 in the blood reacts with H2O to form H2CO3 (role of carbonic anhydrase) • This reaction occurs so rapidly in the RBCs that it reaches almost complete equlibrium within a small fraction of a sec. • Dissociation of H2CO3 into HCO3 and H ion • Most of the H ions combine with hemoglobin • Many of HCO3 ions diffuse from the RBC into the plasma while Cl ions diffuse into the RBCs to take their place • Bicarbonate-chloride carrier protein in the RBC membrane
Transport of Carbon Dioxide • In lung capillaries, bicarbonate ions and hydrogen ions move into RBCs and chloride ions move out. • Bicarbonate ions combine with hydrogen ions to form carbonic acid. • The carbonic acid is converted to carbon dioxide and water. The carbon dioxide diffuses out of the RBCs. • Increased plasma carbon dioxide lowers blood pH. The respiratory system regulates blood pH by regulating plasma carbon dioxide levels
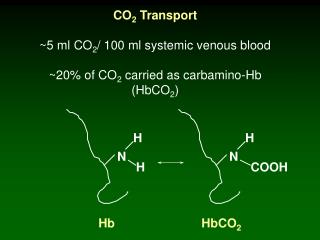
Transport of CO2 in Combination with Hemoglobin and Plasma Proteins • CarbaminoHemoglobin (CO2Hgb) • In addition to reacitng with water, CO2 reacts directly with hemoglobin to form CO2Hgb • This combination of CO2 and hemoglobin is a reversible reaction • A small amount of CO2 also reacts in the same way with the plasma proteins • Carbamino combination with Hgb and plasma proteins is about 23 % of the total quantity of CO2 transported
Haldane Effect • An increase in CO2 in the blood causes O2 to be displaced from hemoglobin (the Bohr Effect) • The reverse is also true: binding of O2 with hemoglobin tends to displace CO2 from the blood (Haldane Effect) • This is quantitatively far more important • The Haldane effect results from the fact that combination of O2 with Hgb in the lungs causes the hemoglobin to become a stronger acid • This displaces CO2 from the blood and into the alveoli
Haldane Effect CO2 dissociation curve
Respiratory Exchange Ratio (R) • Normal transport of O’ from the lungs to the tissues is about 5 ml/100 ml blood • Whereas normal transport of CO2 from the tissues to the lungs is about 4 ml/100 ml blood • Normally, only about 82% as much CO2 is expired from the lungs as O2 is taken up by the lungs • The ratio of CO2 output to O2 uptake is called the respiratory exchange ratio (R)
Respiratory Exchange Ratio • Normal values • CO2 Production = 200 ml/min • O2 Consumption = 250 ml/min • Respiratory exchange ratio is normally less than 1.0. • This means that expiratory minute ventilation is slightly (about 60 ml/min) less than inspiratory minute ventilation.
Respiratory Quotient (RQ) • RQ = (CO2 production) /( O2 utilization) in cell metabolism. • Value changes with substrate utilization • carbohydrates = 1.0 • fats = 0.70 • proteins = 0.80 • average mixed diet = 0.8 • When O2 is metabolized with carbohydrates, one molecule of CO2 is formed for each molecule of O2 consumed • When O2 reacts with fats, a large share of the O2 combines with hydrogen atoms from the fats to form water instead of CO2