Download
1 / 16
160 likes | 301 Views
Engagement and Formal Observation. Trust Policy, History, Context and Interpretation. Engagement and Observation Policy 2014 Historical overview. Original policy written in 2002. Policy consultation process took place across the Trust (service users, carers, staff, managers)

E N D
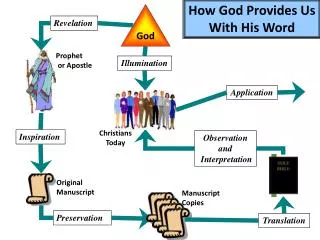
Engagement and Formal Observation. Trust Policy, History, Context and Interpretation
Engagement and Observation Policy 2014 Historical overview • Original policy written in 2002. Policy consultation process took place across the Trust (service users, carers, staff, managers) • New Policy written July 2005, reviewed 2007 policy standards added, training powerpoint, and competency document. Reviewed 2011 (NHSLA) • Move away from `Observation` to `Engagement`. • 2014 Currently being reviewed in light of Professor Len Bowers findings and the implementation of the Care Delivery System (SLaM).
Engagement and observation what the original policy said….. • Reasons why nurses find enhanced observation difficult • Reasons why patients find enhanced observations difficult • Factors related to these:- • Environment • Clinical Skills/ Clinical Leadership • Availability of structure/ activities/ alternatives • Clinical supervision • Boundaries • Expectations
Changes Made…. • Intermittent observations can only be instigated when reducing levels of observations from an enhanced status. • Senior Nurses to be included in the rota for enhanced engagement of patients. • Visual Handover of patients to take place from the shift co-ordinator to the shift co-ordinator on each shift change. • Caringly Inquisitive Behaviour by nurses • Intentional Rounding
Rationale for the changes made in the original policy:- Number 1 • A number of incidents had occurred within the trust on in patient wards • Attempted suicide • Suicide • Self Harm • An audit of all Board Level Inquiries was completed during 2004/5 and any incidents where patients were undergoing `special observations` as they were called then were reviewed. • Many of these incidents occurred whilst patients were undergoing ` 15 minute checks`. Move away from 15 minute checks as patients were able to monitor this quite easily and commit acts of self harm and suicide.
Rationale for changes…Number 2 • Patients who are in need of the most skilled nursing, the most unwell patients are often being cared for by the most junior staff, or by staff who do not know them very well, resulting in limited social or therapeutic conversations. • Patient experiences of enhanced observation described as dehumanising and distressing. (local and national evidence) Some nurses would just sit and read a newspaper, would not talk to the patient, no engagement at all. • Ward managers, deputies, practice development nurses, and other senior nurses will be on the rota for the observation/ engagement with patients. • Encourage role modelling and reflection on practice during the shift.
Rationale for changes…Number 3 • During the review of serious incidents in 2004/5 we found that many of the most serious incidents where patients had harmed themselves or committed suicide were taking place during the handover period between 1-3p.m. • Very few qualified nurses were actually on the ward with the patients. • RMNs were sometimes in the office for a couple of hours before actually seeing a patient, sorting out paperwork, answering the phone, many administrative tasks. • At the beginning of every shift it will be the responsibility of the nurse in charge to carry out a visual handover to the nurse in charge of the next shift, of all the patients on the ward, also the whereabouts of the patients on leave.`
Number 3…..Visual Handover • This is about ensuring that nurses are clear about their level of responsibility when taking over a shift. To know how their patients are, and where they are. • This does NOT replace the verbal handover, but will need to be locally implemented. • `Intentional Rounding`- term used by David Cameron to encourage senior nurses to visually see and monitor patients every hour. • Reassuring for the patients and the Nurse in Charge to be visible at the beginning of the shift.
Intentional Rounding & caringly inquisitive behaviour in the policy…. • Communicating with someone, assessing their mental well being, Being present, helpful, listening, and supportive • A service which is experienced by service users as acceptable, accessible and helpful. • Encourages nurses to be curious and seek out patients who are not attending routine activities, such as groups and meals. • Acknowledges and respects individuals autonomy, identity, strengths and viewpoint. • Attends to wider social needs and aspirations, cares about a person`s `well being`
Changes in Documentation.. • Observation record • Observation care plan • Epjs Observation care plan • Visual Handover recorded on the handover record sheets (some areas completing this now) • Records kept locally of completion of Engagement and Observation competency document, and completion of training. • Current records of intentional rounding to inform ward staff about patients views.
Intermittent Observations… • Patients tolerate intermittent observations better than within arms length or within eyesight observations, and every attempt should be made to reduce levels of observation from within eyesight and within arms length to intermittent as soon as possible. • Engagement with the patient should take place approximately four times an hour, but at irregular intervals, trying to avoid 15 minute checks.
Named levels of observation • Within arms length • Within eyesight • Intermittent • General
Process of reviewing observation levels.. • MDT ( Doctors and Nurses) • Reviewed on each shift. • Changes to levels of enhanced observations can take place when the risk factors have been reduced. This has to be completed and recorded prior to change of status. • Senior clinicians involvement, expertise, advice, • presence on the ward. • Encouraging for junior staff and for patients.
Senior Nurses • Ward managers, deputies, practice development nurses, and other senior nurses will be on the rota for the observation/ engagement with patients. • Encourage role modelling and reflection on practice during the shift. • Reviews of all patients on enhanced levels of observation with Doctors and Nurses.
Resources…. • Multi disciplinary presence on the wards at key handover times, review meetings and community meetings. • Care Delivery System being rolled out across all in patient wards. • Review structures/ activities on the wards. How many patients have a structured activity programme, and how is this maintained. • How are the social areas used to their full advantage • Benefits of skilled activity co-ordinators. • Use of training resources/role plays/ facilitated reflection sessions • Clear philosophy on each ward stating expectations of staff and patients related to specific behaviours. • Nurse Consultant. Supporting Safe and Therapeutic services… how often is this resource being used.
Current policy review includes…. • Adding Caringly Vigilent Behaviour by nurses • Adding Intentional Rounding • Changing the use of Intemittent Observation.Use at any point during the patient admission rather than as a reduction from more enhanced observations.