Download
1 / 39
480 likes | 1.77k Views
EXHALED NITRIC OXIDE IN ASTHMA. DR. MUKHTAR A. ADEIZA DEPARTMENT OF MEDICINE Ahmadu Bello University Teaching Hospital,Zaria Thoracic club meeting, 17 th march 2011. OUTLINE. Introduction History Synthesis of NO Functions of NO Measurement of NO Uses in Asthma Other uses Conclusion.

E N D
EXHALED NITRIC OXIDE IN ASTHMA DR. MUKHTAR A. ADEIZA DEPARTMENT OF MEDICINE Ahmadu Bello University Teaching Hospital,Zaria Thoracic club meeting, 17th march 2011
OUTLINE • Introduction • History • Synthesis of NO • Functions of NO • Measurement of NO • Uses in Asthma • Other uses • Conclusion
Introduction • Asthma is a chronic inflammatory disease of the airways that involves a complex interaction of recurrent episodes of reversible airflow obstruction, bronchial hyperresponsiveness and an underlying inflammation. • Clinical manifestations include: • Episodic wheezing • Coughing • Shortness of breath • Chest tightness
Introduction • In the United States, asthma affects more than 22 million people and is one of the most common chronic diseases of childhood, affecting more than 6 million children. (NHLBI, 2007) • In the United Kingdom, 20% of school age children are affected. • West Africa, 5.7% • Nigeria, 5.4%
Introduction • Decisions regarding asthma management are currently based on symptoms and conventional lung function tests. • Exhaled nitric oxide (FeNO) measured in a breath test has recently emerged as a potentially useful tool in the assessment and management of patients with asthma.
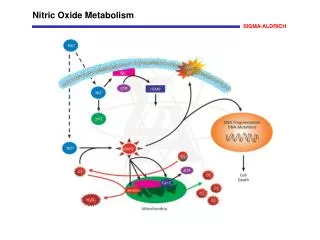
Allergen Macrophage/ dendritic cell Mast cell Th2 cell Neutrophil Eosinophil Mucus plug Epithelial shedding Nerve activation Subepithelial fibrosis Plasma leak Oedema Sensory nerve activation Vasodilatation New vessels Cholinergic reflex Mucus hypersecretion Hyperplasia Bronchoconstriction Hypertrophy / hyperplasia Modern view of asthma Barnes PJ
Nitric Oxide (NO) • NO is a biomarker of eosinophilic airway inflamation. • Produced by the action of proinflammatory cytokines on inducible nitric oxide synthase both in vivo and in vitro.
Properties of NO • Small highly reactive molecule (“radical molecule”) • Made up of one atom each of Nand O • Uncharged with an unpaired electron • Can diffuse freely across membranes • T1/2 is 2-30 seconds • Decays into nitrate after spontaneously transmitting signal
History • 1987, EDRF shown to posesss biological and chemical properties similar to NO. • 1992, NO was named “Molecule of the Year” by the journal Science. • 1998, Furchgott, Ignarro and Murad were awarded the Nobel Prize for Medicine for their work on this molecule.
History • 1990s, numerous authors reported that fractional exhaled nitric oxide concentration (FeNO) was: • Higher in asthmatic patients than in healthy controls. • levels decreased in asthmatic patients treated with inhaled corticosteroids. • Closely linked to eosinophilic airway inflammation.
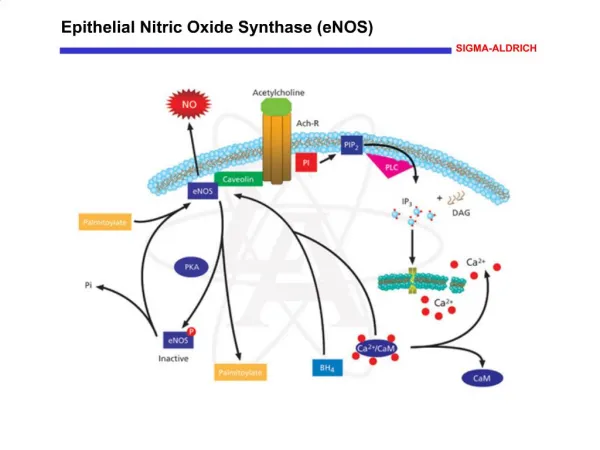
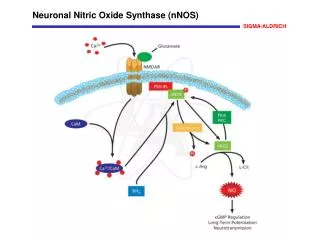
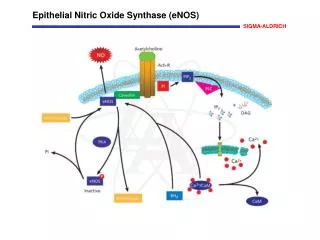
Synthesis of NO • Mammals synthesize NO by way of the NO synthase enzyme (NOS) • NOS converts the amino acid L-arginine into L-citrulline and NO. • The 3 known isoformsof the NOS are classified according to their: • activity, • Location • molecular cloning • Two are constitutive & the third is inducible.
Synthesis of NO L-Arginine ↓ ↓←← iNOS ↓ Nitric Oxide + L-Citrulline
MOA of NO on smooth muscles • NO is an endogenous and diffusible simple free radical that stimulates the enzyme guanylate cyclase. • Increased generation of cyclic guanosine monophosphate (cGMP). • Relaxation of smooth muscles results in bronchodilation and vasodilatation.
Functions of NO • Weak bronchodilator effect. • Vasodilatation. • Neurotransmitter. • Increased host resistance (deaminates DNA). • Upregulates TH2 & Downregulates TH1. • Intensify edema, plasma exudation and cause denudation and desquamation of the epithelial lining.
Factors affecting FeNO levels • Age • Sex • Anthropometry and race • Smoking and diet • Medications • Circadian rhythm & seasonal variation • Others • FeNO decreases after spirometry, sputum induction, bronchoprovocation and within 30mins of exercise.
Measurement of FeNO • PREPATATION • Do not eat, drink, or do strenuous exercise for 1 hour before the test is scheduled. • Do not perform spirometry or peak flow for 1 hour before the test is scheduled. • Continue to take all your medicine as you usually do, unless you have been told to withhold medications for other testing you will be doing.
Procedure • Differ depending on the patients condition: ONLINE: In patients who are able to cooperate, exhale directly. OFFLINE: In patients who are unable to cooperate, exhale into a reservoir. • Single-breath online measurement (SBOL) is the technique of choice in adults and children able to cooperate.
Measurement of FeNO • NO can be measured precisely using chemiluminescence. • NO and ozone react in a cooled chamber to form NO2 . • This photochemical reaction emits infrared light that can be detected by a photomultiplier tube with a linear response.
Procedure • Inhales NO-free air (NO <5 ppb) for 2 to 3 seconds through a mouthpiece. • Exhale completely at a constant flow rate of 50ml/s for 10seconds (ATS, 20005). • Values are then captured and recorded in real time. • A variability of no more than 10% over 3 measurements or no more than 5% over 2 measurements is recommended.
Equipment • NIOX analyzer Standard stationary chemoluminiscence analyzer • NIOX-MINO Based on electrochemical analysis portable hand held device
Reference range • The establishment of reference values for a population is difficult because of the numerous confounding factors as discussed above. • The average normal level of eNO in different studies ranges from 20 to 30 parts per billion.
Refernce range • Olin et al, defined a value of 24.0 to 54.0 ppb depending on age and height. • Abba et al, 7.66 to 46.6 ppb among nonsmoking, nonatopic adult male Saudi subjects.
Clinical application • The availability of cheap, portable and reliable equipment for the measurement of FeNO has led to widespread use of FeNO as a noninvasive diagnostic and management tool particularly in bronchial asthma.
Diagnosis of asthma • Malberg et al. observed that high FENO values ( ≥3SD) correlated with clinical asthma (p<0.0001) • More than 90% specificity for the diagnosis of asthma in both adults and children. • Excellent correlation with esinophilic airway inflammation as represented by blood, sputum, and mucosal esinophilia.
Diagnosis of asthma • Higher diagnostic sensitivity (88%) when compared to various LFTs like induced sputum (86%) and forced spirometry (47%). • Atopy limits the clinical utility of the test in children.
Monitoring of asthma • Monitor antiinflammatory treatment with ICS. • Identify patients who will respond to ICS (FeNO >47ppb). • When tailoring ICS dose in asthma, mean daily dose if ICS was lower in the FeNO group compared to symptoms/spirometry.
Conclusion • FeNO measurements arequick and easy to perform and may be readily incorporated intoroutine pulmonary function test procedures. • This advance offersthe possibility that a diagnosis of asthma may be performedmore easily and confirmed with much greater confidence thanhas been possible to date.
Conclusion • The possibility of easily taking measurements of FeNO in an office setting even by relatively young children, and the availability of a portable device, opens a significant perspective for the routine use of FeNO evaluation in daily practice.
The future • Development of local reference values • Integration of FeNO use into medical practice in both primary care and specialist settings in Nigeria.