Download

1 / 14
160 likes | 354 Views
Rocky Mountain Spotted Fever. Pat Barrett Morning Report July 2, 2010. Rickettsia rickettsii (facts you probably know). Tick borne, though 1/3 to 1/2 do not recall a tick bite Dermacentor variabilis tick Incidence 15/100,000 persons at the most endemic areas

E N D
Rocky Mountain Spotted Fever Pat Barrett Morning Report July 2, 2010
Rickettsiarickettsii(facts you probably know) • Tick borne, though 1/3 to 1/2 do not recall a tick bite • Dermacentor variabilis tick • Incidence 15/100,000 persons at the most endemic areas • 1-3% ticks infected in endemic areas MMWR: 2006: 55RR04: 1
Pathophysiology • Gram negative intracellular • Virulence depends on the status of the vector • Trophic for endothelial cells • Transits rapidly by activating actin within host’s cells • No exotoxins, will cause necrosis, lymphohistiocyticvasculitis
Incidence of RMSF CDC /epidemiology
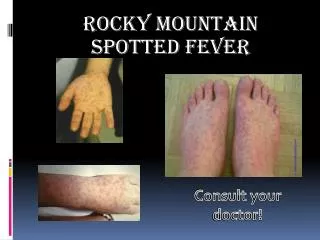
Symptoms Usually develop 5-7 days after tick exposure Fever, headache, myalgia, arthralgia, nausea, vomiting Spotless RMSF occurs approx 10% of the time
RMSF Rash • Typically at 5-7 days • Begins on wrists, ankles, palms and soles, then spreads centripetally • Often macularpapular then petechial • Rarely pruritic
Spotless RMSF • Case Series from Duke (1) • 61% male • 66% African American • 53% mortality in the case series • 22.9% mortality in separate case series (2) where treatment was delayed past 5 days • 6.5% mortality if treated w/in 5 days 1: Clin Infect Dis 1992: 15:439 2: Clin Infect Dis 1995: 20:1118
Laboratory Data • Clinical impression followed by acute and convalescent sera • Typically the latex agglutination has the fastest turn around time • IFA test for IgG and IgM, felt to be the standard, used by CDC. • False positives w/ other rickettsial exposures • PCR not widely available • Also hyponat, elevated transaminases, prolonged PT, aPTT
Is There a Best Test? Am J Trop Med Hyg: 1986: 35: 840 Gold Standard: 4 fold increase from acute to convalescent, convalescent IFA > 1:64, isolation of Rickettsiae, fluorescent ab of specimen from bx or autopsy Indirect hemagglutination 94% sens Indirect fluorescent antibody 96% sens Latex agglutination 71% sens
Is There A Best Therapy? J Clin Microbiol 1978;8:102 Doxycycline 7 days, 10-14 in severe cases 2nd Line Chloramphenicol No preventive therapy recommended for tick bites w/o illness – shown to delay symptom onset but not prevent infection.
Conclusions • Ticks are awful • RMSF and Ehrlichia should be considered during any FUO work-up while a resident at UNC • There is some variability in when serology is positive • Rashless and rashalittle RMSF does exist • The benefits of not treating empirically must be carefully weighed against the risks
References • NC DHHS: http://www.epi.state.nc.us/epi/gcdc/pdf/cdtable2009.pdf • CDC/epidemiology: http://www.cdc.gov/ncidod/dvrd/rmsf/epidemiology.htm • Chapman, AS et. MMWR: 2006: 55RR04: 1 • Up To Date: RMSF • Sexton, DJ, et al. Clin Infect Dis 1992: 15:439 • Kirkland, KB, et al. Clin Infect Dis 1995: 20:1118 • Kaplan, JB, et al. Am J Trop Med Hyg: 1986: 35: 840 • Kenyon RH, Williams RG, Oster CN, Pedersen CE Jr. Prophylactic treatment of Rocky Mountain spotted fever. J ClinMicrobiol 1978;8:102--4.