Download
1 / 124
1.29k likes | 2.95k Views
Sleep Apnea. Dr. Vishal Sharma. History. Lugaresis (1970): described OSAS Stanford University (1972): Polysomnography Sleep Latency Test devised in 1976 Before 1980’s tracheostomy main treatment Ikematsu performed first UPPP in 1952 Fujita popularized UPPP

E N D
Sleep Apnea Dr. Vishal Sharma
History Lugaresis (1970): described OSAS Stanford University (1972): Polysomnography Sleep Latency Test devised in 1976 Before 1980’s tracheostomy main treatment Ikematsu performed first UPPP in 1952 Fujita popularized UPPP Kamami developed LAUP in late 1980s
Sleep related breathing disorders Synonym: sleep disordered breathing Consists of: A. Snoring B. Obstructive sleep apnea C. Obstructive sleep hypopnea D. Upper airways resistance syndrome
Arousal:Abrupt change from deep stage to lighter stage of NREM sleep, or from REM sleep to awakening Arousal index:Number of arousals per hour of sleep Apnea:Cessation of breathing for > 10 seconds Apnea Index:Number of apneas per hour of sleep Hypopnea:Decreased airflow (>50%) with oxygen desaturation (> 4% ) for > 10 seconds Snoring:breathingnoise due to partial upper airway obstruction
Obstructive sleep apnea:Cessation of airflow for > 10 seconds even with continued respiratory effort Obstructive sleep hypopnea:Decreased airflow (>50%) with oxygen desaturation (> 4% ) for > 10 seconds even with continued respiratory effort Upper airway resistance syndrome (respiratory effort related arousal):partial airway obstruction with no apnea or hypnea, but arousal index > 15
Respiratory Distress Index: Number of apneas + hypopneas + respiratory effort related arousals per hour Obstructive sleep apnea syndrome: 30 or more episodes of obstructive sleep apnea during a 7- hour period of sleep or apnea index > 5 or respiratory distress index > 15
Types of sleep apnea 1. Obstructive:Normal respiratory chest wall movement 2. Central:No respiratory chest wall movement 3. Mixed:Partial respiratory chest wall movement
Grades of sleep apnea American Sleep association grading: 1. Mild ------------ 5 - 20 apneas per hour 2. Moderate ----- 20 - 40 apneas per hour 3. Severe -------- more than 40 apneas per hour
Cheyne-Stokes breathing-central sleep apnea due to renal failure, heart failure, stroke • Diabetes mellitus, Hypothyroidism, Acromegaly, Parkinson disease, Myasthenia gravis, Idiopathic cardiomyopathy, Muscular dystrophy • Medullary tumor or infarction • Arnold-Chiari malformation • Cervical cordotomy • High-altitude periodic breathing (at > 5000m) • Use of opiates & other CNS depressants
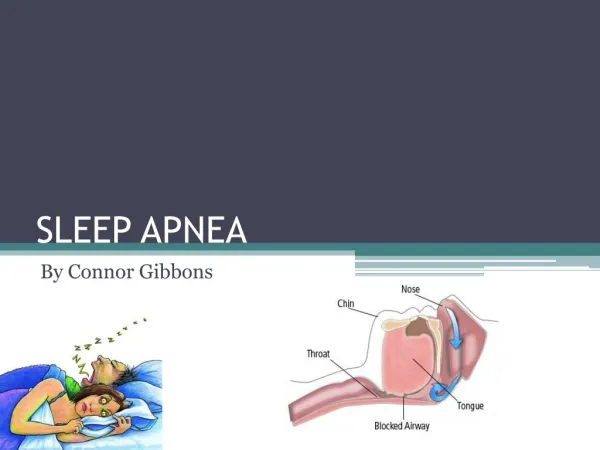
Nose Nasal polyps DNS ed Turbinate Nasal packing Larynx Tumors Edema Stenosis Pharynx Nasopharyngeal tumor Adenoids ed palatal / lingual tonsil Enlarged lingual tonsils Retropharyngeal mass Large tongue Micrognathia / Retrognathia Obesity
Increased compliance of pharyngeal tissues + Neuromuscular in-coordination & ed muscle tone + Anatomical abnormalities Upper airway collapse airway obstruction Hypoxia + negative intra-thoracic pressure Arousal Increased tone of upper airway muscles + upper airway obstruction clears Patient goes to sleep Upper airway collapses again causing arousal
Complications of sleep apnea Systemic hypertension Coronary artery disease Pulmonary hypertension Right heart failure Cardiac arrhythmias Cerebro-vascular accident Polycythemia Sleepiness accidents Depression Impotence Vagal bradycardia Sudden nocturnal death
Symptoms of sleep apnea Day- time Excessive sleepiness Morning headache Intellectual deterioration Personality change Depression Xerostomia Abnormal movements Night- time Snoring Observed choking Arousal from sleep Repeated waking Nocturnal sweating Nocturnal enuresis Impotence
Typical OSAS patient • Synonym: Pickwickian syndrome • Middle age or elderly male with hyper somnolence • Obese with body mass index > 30 • Short neck with its circumference > 17 inches • Hypertension & right heart failure • Large bulky tongue, hypertrophied tonsils, bulky soft palate, prominent posterior pharyngeal wall rugae
History from sleep partner • Bed timings • Body position • Snoring • Apnea (choking) • Arousal from sleep • Alcohol consumption • Sedative use
Epworth daytime sleepiness scale Score > 16 = moderate to severe sleep apnea
Physical examination General appearance, weight, body mass index Blood pressure, cardiovascular examination Cranio-facial: retrognathia, hypoplastic maxilla Nasal: airway patency, DNS, turbinate hypertrophy Tongue: macroglossia, lingual tonsil Nasopharynx: adenoids, polyp, cyst, tumor
Physical examination Oropharynx: Soft palate, palatine tonsil, base of tongue, posterior pharyngeal wall Hypopharynx: tumor Larynx: cyst, tumor, vocal cord mobility Neck: short wide neck (circumference > 17 inches) Thyroid enlargement, features of hypothyroidism
General Investigations • Complete blood count: anemia, polycythemia • Chest x-ray: cardiomegaly, pulmonary disorder • Lung function:portable spirometry flow volume loop saw-tooth pattern • Thyroid function tests: hypothyroidism • Electro-cardiography: cardiac arrhythmias • Arterial blood gas analysis
Investigations for confirmation of sleep apnea • Polysomnography • Portable sleep monitoring • Overnight pulse oximetry recording • Multiple sleep latency test
Polysomnography parameters 1. Electro-encephalogram (EEG) 2. Electro-myogram (EMG): submental, anterior tibialis 3. Electro-oculogram (EOG) / Electro-nystagmogram 4. Electro-cardiogram (ECG) 5. Oxygen saturation 6. Nasal & oral airflow 7. Chest + abdominal movement detector 8. Sleeping position detector 9. Tracheal microphone 10. Esophageal manometer
Investigations to assess site of airway obstruction Awake patientSleeping patient Muller maneuverFlexible nasendoscopy Lateral cephalometrySomno-fluoroscopy C.T. scan of neck Cine C.T. scan Pharyngeal manometry
Muller’s maneuver • After a forced expiration, pt attempts inspiration with closed mouth & nose, whereby negative pressure leads to collapse of airway • Previously introduced flexible endoscope (via nasal cavity) identifies weakened sections of airway at levels of soft palate & tongue base, during this maneuver
Muller’s maneuver in snoring shows no airway narrowing Before Muller After Muller
Muller’s maneuver in apnea shows airway narrowing Before Muller After Muller