Download
1 / 67
740 likes | 1.33k Views
Chapter 26: The Urinary System. An Introduction to the Urinary System. Figure 26–1. 3 Functions of the Urinary System. Excretion : removal of organic wastes from body fluids Elimination : discharge of waste products Homeostatic regulation :

E N D
An Introduction to the Urinary System Figure 26–1
3 Functions of the Urinary System • Excretion: • removal of organic wastes from body fluids • Elimination: • discharge of waste products • Homeostatic regulation: • of blood plasma volume and solute concentration
Kidneys Urinary Tract • Organs that eliminate urine: • ureters (paired tubes) • urinary bladder (muscular sac) • urethra (exit tube) • Organs that excrete urine Urination or Micturition • Process of eliminating urine • Contraction of muscular urinary bladder forces urine through urethra, and out of body
5 Homeostatic Functions of Urinary System • Regulate blood volume and blood pressure: • by adjusting volume of water lost in urine • releasing erythropoietin (increase RBC production) and renin (regulates blood pressure) • Regulate plasma ion concentrations: • sodium, potassium, and chloride ions (by controlling quantities lost in urine) • calcium ion levels (through synthesis of calcitriol) • Help stabilize blood pH: • by controlling loss of hydrogen ions and bicarbonate ions in urine
Conserve valuable nutrients: • by preventing excretion while excreting organic waste products • Assist liver to detoxify poisons
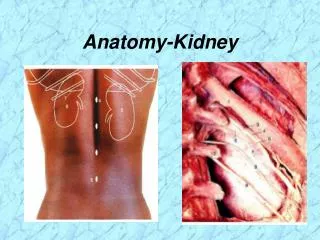
The Position of the Kidneys • Are located either side of vertebral column: • left kidney lies superior to right kidney • superior surface capped by adrenal gland • Position is maintained by: • overlying peritoneum • contact with adjacent visceral organs • supporting connective tissues Figure 26–2
Typical Adult Kidney • Is about 10 cm long, 5.5 cm wide, and 3 cm thick • Weighs about 150 g
Hilum • Point of entry for renal artery and renal nerves • Point of exit for renal vein and ureter
Renal Sinus • Internal cavity within kidney • Lined by fibrous renal capsule
Renal Capsule • Bound to outer surfaces of structures in renal sinus • Stabilizes positions of ureter, renal blood vessels, and nerves
Renal Cortex • Superficial portion of kidney in contact with renal capsule • Reddish brown and granular
Renal Lobe • Consists of: • renal pyramid • overlying area of renal cortex • adjacent tissues of renal columns • Produces urine
Renal Papilla • Ducts discharge urine into minor calyx: • cup-shaped drain
Major Calyx • Formed by 4 or 5 minor calyces
Renal Pelvis • Large, funnel-shaped chamber • Consists of 2 or 3 major calyces • Fills most of renal sinus • Connected to ureter, which drains kidney
Functional Anatomy of Nephron & Collecting System Figure 26–6
Nephron • Consists of renal tubule and renal corpuscle • Microscopic, tubular structures in cortex of each renal lobe • Where urine production begins
Renal Tubule • Long tubular passageway • Begins at renal corpuscle Renal Corpuscle • Spherical structure consisting of: • Bowman’s capsule • cup-shaped chamber • capillary network (glomerulus)
Filtration • Occurs in renal corpuscle • Blood pressure: • forces water and dissolved solutes out of glomerular capillaries into capsular space • produces protein-free solution (filtrate) similar to blood plasma
3 Functions of Renal Tubule • Reabsorb useful organic nutrients that enter filtrate • Reabsorb more than 90% of water in filtrate • Secrete waste products that failed to enter renal corpuscle through filtration at glomerulus
Cortical and Juxtamedullary Nephrons Figure 26–7
Cortical Nephrons (1 of 2 types) • 85% of all nephrons • Located mostly within superficial cortex of kidney • Loop of Henle is relatively short • Efferent arteriole delivers blood to a network of peritubular capillaries: • which surround entire renal tubule
The Renal Corpuscle • Each renal corpuscle: • is 150–250 µm in diameter • includes Bowman’s capsule and glomerulus
Filtration • Blood pressure: • forces water and small solutes across membrane into capsular space • Larger solutes, such as plasma proteins, are excluded Filtration at Renal Corpuscle • Is passive • Solutes enter capsular space: • metabolic wastes and excess ions • glucose, free fatty acids, amino acids, and vitamins
Reabsorption • Useful materials are recaptured before filtrate leaves kidneys • Reabsorption occurs in proximal convoluted tubule
The Thick Descending Limb • Ascending Limbs • Of juxtamedullary nephrons in medulla: • create high solute conc. in peritubular fluid • Has functions similar to PCT: • pumps sodium & chloride ions out of tubular fluid • The Thin Segments • Are freely permeable to water, not to solutes • Water movement helps conc. tubular fluid • The Thick Ascending Limb • Ends at a sharp angle near the renal corpuscle - where DCT begins
3 Processes of the DCT • Active secretion of ions, acids, drugs, and toxins • Selective reabsorption of sodium and calcium ions from tubular fluid • Selective reabsorption of water: • concentrates tubular fluid
Transports tubular fluid from nephron to renal pelvis • Adjusts fluid composition • Determines final osmotic concentration and volume of urine
Renal Physiology • The goal of urine production: • is to maintain homeostasis • by regulating volume and composition of blood • including excretion of metabolic waste products • Urea • Due to breakdown of aa • Creatinine • Due to breakdown of creatinine kinase (important in muscle contraction) • Uric acid • Formed due to recycling of ATGCU
Organic Waste Products • Are dissolved in bloodstream • Are eliminated only while dissolved in urine • Removal is accompanied by water loss • Concentrated urine: • 1200–1400 milliosmols/L (4 times plasma concentration)
Differences between Solute Concentrations in Urine and Plasma Table 26–2
3 Basic Processes of Urine Formation • FILTRATION • Hydrostatic pressure forces water through membrane pores: • small solute molecules pass through pores • larger solutes & suspended materials are retained • Occurs across capillary walls: • as water and dissolved materials are pushed into interstitial fluids • In some sites (ie –liver), pores are large: • plasma proteins can enter interstitial fluids • At the renal corpuscle: • specialized mem. restricts all circulating proteins
2 & 3 Reabsorption and Secretion • At the kidneys involve: • Diffusion– passive molecular movement from an area of high conc to area of low conc • Osmosis-movement of water across semi-perm mem from area of low conc of solute to higher con of solute • channel-mediated diffusion- specific channel used, no energy, conc. dependent • carrier-mediated transport – next slide
The Transport Maximum(Tm) • Concentration higher than transport maximum: • exceeds reabsorptive abilities of nephron • some material will remain in the tubular fluid and appear in the urine • Determines the renal threshold • the plasma concentration at which: • a specific compound or ion begins to appear in urine
Renal Threshold for Glucose • Is approximately 180 mg/dl • If plasma glucose is greater than 180 mg/dl: • Tm of tubular cells is exceeded • glucose appears in urine Glycosuria • Is the appearance of glucose in urine
Renal Threshold for Amino Acids • Is lower for glucose (65 mg/dl) • Amino acids commonly appear in urine: • after a protein-rich meal Aminoaciduria • Is the appearance of amino acids in urine
Aldosterone • Is a hormone produced by adrenal cortex • Reduces Na+ lost in urine Hypokalemia • Produced by prolonged aldosterone stimulation • Dangerously reduces plasma concentration Natriuretic Peptides • Oppose secretion of aldosterone
Parathyroid Hormone and Calcitriol • Circulating levels regulate reabsorption at the DCT
Acidosis • Lactic acidosis: • develops after exhaustive muscle activity • (bulging muscles can cut off blood supply) • due to anaerobic respiration • Ketoacidosis: • Lower blood pH, higher acid, due to presence of ketones • develops in starvation or diabetes • Body does not have suff. glucose/glycogen to sustain met activity • Muscle loss can occur - dieting
Control of Blood pH • By H+ removal and bicarbonate production at kidneys • Is important to homeostasis Alkalosis • Abnormally high blood pH • Can be caused by prolonged aldosterone stimulation: • which stimulates secretion
Response to Acidosis • PCT and DCT deaminate amino acids: • ties up H+ • yields ammonium ions (NH4+) and HCO3—(carbonic acid) • Ammonium ions are pumped into tubular fluid • Bicarbonate ions enter bloodstream
ADH – antidiuretic hormone • Hormone causes special water channels to appear • Increases rate of osmotic water movement • Higher levels of ADH increases: • number of water channels • water permeability of DCT and collecting system • No ADH, water is not reabsorbed • All fluid reaching DCT is lost in urine producing large amounts of dilute urine
The Hypothalamus • Continuously secretes low levels of ADH: • At normal ADH levels: • collecting system reabsorbs 16,800 ml fluid/ day (9.3% of filtrate) • A healthy adult produces: • 1200 ml urine per day (0.6% of filtrate)
Diuretics • Are drugs that promote water loss in urine (diuresis) • Diuretic therapy reduces: • blood volume • blood pressure • extracellular fluid volume
The Composition of Urine • Results from filtration, absorption, and secretion activities of nephrons • Some compounds (such as urea) are neither actively excreted nor reabsorbed along nephrons • Organic nutrients are completely reabsorbed: • other compounds missed by filtration process (e.g., creatine)
The Concentration of components • in a urine sample depends on osmotic movement of water • Normal Urine • Is a clear, sterile solution • Yellow color (pigment urobilin) generated in kidneys from urobilinogens
A Summary of Renal Function Figure 26–16a
Step 1: Glomerulus • Filtrate produced at renal corpuscle has the same composition as blood plasma: • without plasma proteins
Step 2: Proximal Convoluted Tubule (PCT) • Active removal of ions and organic substrates: • produces osmotic water flow out of tubular fluid • reduces volume of filtrate • keeps solutions inside and outside tubule isotonic