Download
1 / 26
300 likes | 536 Views
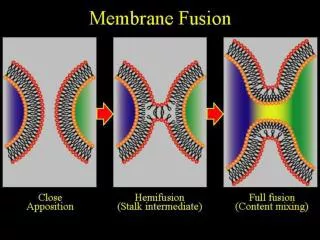
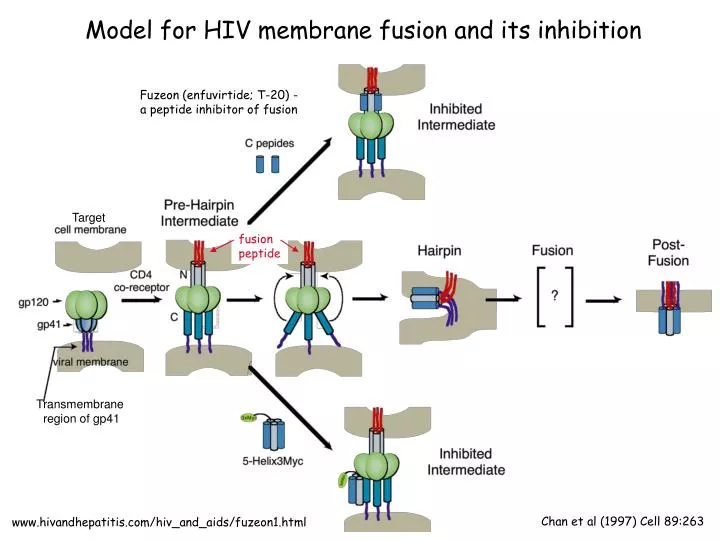
Fuzeon (enfuvirtide; T-20) - a peptide inhibitor of fusion. Model for HIV membrane fusion and its inhibition. Target. fusion peptide. Transmembrane region of gp41. Chan et al (1997) Cell 89:263. www.hivandhepatitis.com/hiv_and_aids/fuzeon1.html.

E N D
Fuzeon (enfuvirtide; T-20) - a peptide inhibitor of fusion Model for HIV membrane fusion and its inhibition Target fusion peptide Transmembrane region of gp41 Chan et al (1997) Cell 89:263 www.hivandhepatitis.com/hiv_and_aids/fuzeon1.html
Review of HIV lifecycle and sites of drug actions Note: gp120 undergoes a major conformational change after binding CD4. There are no current data addressing whether it also undergoes a conformational change after binding CCR5. Also, gp41 is not as elongated or accessible as depicted here, immature viruses that bud from cells don’t yet contain bullet-shaped cores, and HIV virions contain only ~14 envelope spikes.
HIV reverse transcriptase -- Two enzymes in one After building a DNA strand from the RNA template using polymerase activity, the RNase activity destroys the RNA strand, then a second DNA strand is constructed from the first by the polymerase. http://www.rcsb.org/pdb/static.do?p=education_discussion/molecule_of_the_month/pdb33_2.html
Crystal structure of HIV RT bound to Nevirapine, a NNRTI that binds near, but not in, the polymerase active site PDB code 1jlb The PDB contains >100 RT/inhibitor complexes. http://www.rcsb.org/pdb/static.do?p=education_discussion/molecule_of_the_month/pdb33_2.html
Catalytic domain of HIV integrase Integrase is a target of anti-HIV drugs Drugs targeting HIV integrase are being tested: e.g., MK-0518 (Raltegravir), Elvitegravir, GS-9137. Some are in clinical trials.http://www.hivandhepatitus.com/recent/experimental_drugs/docs/intergrase.html http://www.medscape.com/viewarticle/417310 http://adrik.bchs.uh.edu/publicity/integrase/choe.html
Summary of HIV lifecycle(emphasis on integrase and integration)
Natural substrate Structure-based drug design was used to make HIV protease inhibitorshttp://publications.nigms.nih.gov/structlife/chapter4.html# HIV protease is a 2-fold symmetric dimer with one active site. HIV protease’s natural substrate is asymmetric. Drug-resistant mutations in HIV protease Design 2-fold symmetric drug candidate molecules.
Indinavir Structure-based drug design -- an engineering project • If you know: • The 3D structure of a protein to high resolution (usually determined by X-ray crystallography) • The site you need to block (usually the active site if the protein is an enzyme) • The relative energies contributed by different types of binding interactions Then you can (in theory) design an inhibitor to that protein. Structure-based drug design needs structural biologists, computer scientists, physicists, and chemists.
HIV reverse transcriptase has no proof-reading activity • In vivo mutation rate is ~1/33,000 nucleotides/replication cycle* (1/107 for DNA polymerase; 1/109 including mismatch repair). • The exceptional diversity of the HIV-1 genome results from error-prone reverse transcription. • Most of the mutant viruses are inferior or not viable, but some are better than the parental virus at escaping from the immune system or from anti-viral drugs. Natural selection at work! • Error rates of ~1/1700 nucleotides in in vitro assays; base substitution, addition, deletion errors (Manksy & Temin, 1995, J Virol. 69: 5087-94; Roberts et al., 1988, Science 242: 1171-1173).
What is the problem with mutations? • Genetic changes are what drive evolution -- they allow organisms to adapt to changing conditions and colonize new habitats. • BUT … from the perspective of a single organism (e.g., you or me), a permanent genetic change (mutation) can have profoundly negative consequences: • Sickle cell anemia, an inherited disease, is caused by a change in one nucleotide leading to a single amino acid change in hemoglobin. • Cancers are caused by a gradual accumulation of random mutations in DNA of somatic* cells. • From the perspective of a virus, mutations are great because they allow emergence of rare variants that have increased fitness and/or can evade the host immune system more effectively. *Somatic cells are all the cells in an organism other than germ cells (the reproductive cells).
Resistance of HIV to a single protease inhibitor Viral RNA levels initially fall after administering a single protease inhibitor. Combinations of drugs are needed for long term decrease of viral load CD4 T cell count rises, but then falls as virus levels rise. Many new variants of HIV in a single person every day leads to drug resistance. HIV replication rate: 109-1010 virions/day. - Mutation rate: ~ 3 x 10-5/nucleotide base/replication cycle. Genome size is 104 bases. At least one mutation can occur in each nucleotide of HIV in a single day. Treatment involves combination anti-retroviral drug therapy: HAART -- highly active anti-retroviral therapy. Current HAART formulations are combinations of viral protease and reverse transcriptase inhibitors. Future HAART regimens may involve entry, fusion, and/or integrase inhibitors. After only four weeks, 100% of HIV is drug-resistant; T cell counts back down. Figure 11.27. Janeway et al. Immunobiology
Anti-retroviral therapy hasn’t eradicated HIV Anti-retroviral treatment regimens are complex, expensive, and can result in serious side effects. However, anti-retroviral drugs can easily and effectively block mother-to-child transmission (next slide). Developing safe, effective and affordable vaccines that can prevent HIV infection in uninfected people is the best hope for controlling and/or ending the AIDS epidemic. In 1984, Margaret Heckler (President Reagan’s Secretary of the Department of Health and Human Services) announced that the virus responsible for causing AIDS had been identified, and that a vaccine would be ready for testing within two years. We still don’t have a vaccine. To understand why, you need to learn about the host immune system and how other viruses trigger effective immune responses.
Transmission rate of HIV from mother to child: 30-35% 2/3 of transmission during birth; 1/3 during breast feeding Drug therapy: 4 weeks of AZT before birth plus nevirapine at birth blocks transmission (both are reverse transcriptase inhibitors) US & Europe: <2% of babies born to HIV-positive mothers get the virus (nearly complete access to drugs) World-wide: ~11% of HIV-positive pregnant women have access to drugs to block transmission ~12% of new HIV infections every year are due to mother-child transmission
Labeling techniques for immunofluorescence microscopy and flow cytometry Kuby, Kindt, Goldsby, Osborne Immunology Textbook
Flow cytometry --Fluorescence Activated Cell Sorting (FACS) A- cells A+ cells Single color FACS analysis (e.g., using anti-A antibody) -- note this is a log scale A two-color FACS analysis Kuby, Kindt, Goldsby, Osborne Immunology Textbook
Stanford used flow cytometry to screen blood before HIV tests were available Reduced ratio of CD4+ to CD8+ T cells in AIDS patients July 1983 to June 1985, Stanford Blood Center used flow cytometry to test donated units for CD4:CD8 ratio Did not transfuse blood from donors with CD4:CD8 ratio < 0.85 Most other blood banks did no screening ~10,000 cases of transfusion-transmitted AIDS in US before HIV test available in 1985 Galel et al., 1995, “Prevention of AIDS transmission through screening of the blood supply” Annu. Rev. Immunol. 201-227
Killing viruses • Can inactivate viruses using physical and chemical agents • Heat (e.g., boiling water) alters structures of proteins and nucleic acids • UV radiation crosslinks thymines in nucleic acids • Formaldehyde combines with free amino groups on nucleic acids • Metals and phenol react with proteins in the viral capsid • Chlorine combines chemically with viral nucleic acid • Detergents denature viral proteins • Antiviral drugs (rare because they can interfere with essential chemical reactions in the host)
Transmission of HIV Having unprotected sexual contact such that sexual secretions of one partner come into contact with the genital, oral, or rectal mucous membranes of the other partner. Transfusion of contaminated blood (donated blood is now screened and blood products are heat-treated to destroy HIV). Transfer of blood in contaminated needles. Mother to child transmission during pregnancy, birth or breast-feeding. HIV is NOT transmitted by Kissing. Shared food utensils, towels, bedding, swimming pools, toilet seats, mosquitos, bedbugs.
Typical transmission of HIV through sex DCs serve as a “Trojan Horse” for HIV, because they transport it to a place where it can infect T cells. This is an excellent example of how HIV has usurped an immune function meant to protect the host (patrolling of mucosal surfaces by DCs) for its own purposes. DCs are supposed to uptake pathogens, degrade them, and present pieces of them to T cells in order to trigger an immune response. R5 HIV viruses (usually in semen) reach mucosal epithelial cells that line the male and female genital tracts. HIV gains access to dendritic cells (DCs) at sites of mucosal injury, or to DCs that are sampling the external world by protruding between epithelial cells. HIV gp120 binds to a DC protein, DC-SIGN, and then gets endocytosed into early endosomes (receptor-mediated endocytosis). HIV survives the acidic pH of early endosomes instead of being degraded. DCs migrate to lymph nodes where there are a lot of CD4 T cells. HIV translocates to the DC cell surface and is transferred to a CD4 T cell, which it infects by fusing to the plasma membrane. Figure 11.22; Janeway et al., Immunobiology: the immune system in health and disease, 6th edition
Cell types infected by HIV are determined by which chemokine receptor is used as a coreceptor • HIV variants found in primary infections (R5 viruses) use CCR5 and require only low levels of CD4. In addition to CD4 T cells, R5 viruses can infect dendritic cells* and macrophages* in vivo. • Infected dendritic cells initiate infection by transporting HIV from mucosal surfaces to lymphoid tissues, where viruses can infect CD4 T cells. • Other HIV variants (X4 viruses) use CXCR4 and only infect CD4 T cells in vivo. X4 viruses require high levels of CD4 on the target cell for infection. • Late in infection, the viral phenotype switches from R5 to X4 (viruses that uses CXCR4 coreceptors) in 50% of cases. This switch is associated with a rapid decline in CD4 T cells and progression to AIDS. Dendritic cells and macrophages are cells that present antigens (e.g., viruses and bacteria) to the immune system.
What should you target to make an anti-viral drug? • An activity that is critical for viral function • An activity that is virally-encoded • An activity that is not similar to host activities • but RT is a polymerase similar to host polymerases… • Fortunately NRTIs and NtRTIs bind RT more tightly (higher affinity) than they bind DNA polymerase. • Also if they did get incorporated by DNA polymerase, NRTIs would be removed from host cell DNA during DNA repair. • HOWEVER -- mitochondrial DNA is replicated by polymerase gamma, which binds NRTIs, so mitochondrial DNA can be damaged, resulting in cell death due to low energy production. • Different NRTIs affect mitochondria of different types of cells, so have different side effects.
Side effects of some reverse transcriptase inhibitors include: • Headaches, high blood pressure, nausea, vomiting, fatigue (can disappear with time) • Less frequent, but more serious side effects include anemia (shortage of red blood cells), myopathy (muscle pain and weakness), neutropenia (low number of neutrophils) Note: RT inhibitors are usually used in combination with other types of anti-retroviral drugs (protease or fusion inhibitors).
Reverse transcriptase inhibitorsRT inhibitors prevent synthesis of double stranded viral DNA, thus prevent HIV from multiplying • Nucleoside analog RT inhibitors (NARTIs or NRTIs) • Competitive substrate inhibitorsLacks 3’ OH so causes chain terminationExample: AZT, the first anti-HIV drug • Conversion to nucleotide by phosphorylation in body can cause toxicity • Nucleotide analog RT inhibitors (NtARTIs or NtRTIs) • Competitive substrate inhibitorsLacks 3’ OH so causes chain termination • Doesn’t need to be converted by body, soless toxic • Non-nucleoside RT inhibitors (NNRTIs) • Non-competitive substrate inhibitors • Not incorporated into viral DNA • Inhibit polymerase through conformational changes in active site
FDA-approved reverse transcriptase inhibitors http://www.hivandhepatitis.com/hiv_and_aids/hiv_treat.html