Download
1 / 53
590 likes | 1.25k Views
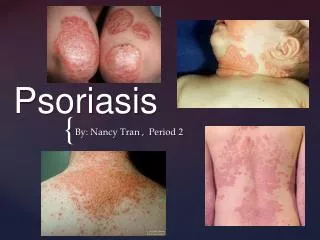
Psoriasis. Psoriasis is a non-infectious, chronic inflammatory disease of skin, characterized by well defined erythematous plaques with silvery scale. Occurs mostly over extensor surfaces and scalp. Characteristic Lesion of Psoriasis!. Histopathology

E N D
Psoriasis is a non-infectious, chronic inflammatory disease of skin, characterized by well defined erythematous plaques with silvery scale. • Occurs mostly over extensor surfaces and scalp.
Histopathology • Increased epidermal cell proliferation due to :increased growth fraction,shorten epidermal turnover time normal 60 to10 days • Thickening of the epidermis(acanthosis)with suprapapilary thinning responsible for the Ausitz sign) • Retention of nuclei by keratinocytes (parakeratosis) • Collection of polymorphs in the epidermis forming micro a microabscesses • Tortuous and dilated blood vessels • Inflammatory infiltrate primarily of lymphocytes in the upper dermis • Prolifilation of fibroblast
Precipitating factors! • Trauma • Appears in areas of skin damage like scratches or surgical wounds (Koebner phenomenon) • Infection • Preceded by β-hemolytic streptococcal throat infection (Guttate),HIV • Sunlight • Rarely, ultraviolet radiation may worsen psoriasis • Drugs • Antimalarials, β-blockers and lithium- worsens psoriasis • Stopping systemic steroids- rebound of psoriasis • Emotion • Anxiety precipitates some exacerbations
cause and Pathogenesis! • The exact cause is still unknown • T-cell mediated inflammatory disease • Epidermal hyperproliferation secondary to activation of immune system • Altered maturation of skin • Inflammatory cell infiltrate with neutrophilic and lymphocytic predominance. • Vascular changes • Cause: Excessive number of germinative cells entering the cell cycle rather than by a decrease in cell cycle time. • The turnover is greatly shortened, to less than 10 days as compared to a normal turnover period of 60 days
Associated Factors • Genetic Factors: - 30% of people with psoriasis have had psoriasis in family • Nongenetic Factors: - Mechanical, ultraviolet, chemical injury - Infections: Strep, viral, HIV - Prescription Drugs, stress, endocrine, hormonal, obesity, alcohol, smoking
GENETICS • Affected Parent Chance of developing • 1 of the parent affected 15% • Both are affected 50% • If one sibling already has the disease The chance still goes higher • The risk of those with HLA-Cw6 genotype developing psoriasis is 10-20 times more than those without it.
Psoriasis occurs in 2% of the world’s population. • Highest in Caucasians • In Africans, African-Americans and Asians- between 0.4% and 0.7% • Equal frequency in males and females • May occur at any age- from infancy to the 10th decade of life. Mostly occurs at the age of 10 or more.
Prevalence! • Two-thirds of patients have mild disease • One-third have moderate to severe disease • Early onset (prior to age 15) • Associated with more severe disease • More likely to have a positive family history • Life-long disease • Remitting and relapsing unpredictably • Spontaneous remissions of up to 5 years have been reported in approximately 5% of patients
Sharply demarcated erythematous plaque with silvery white scale
Presentation pattern of psoriasis Differntial diagnosis Drug eruption,lichen planus Pityriasis rosea Candidiasis of flexures Hyperkeratotic eczema,sebhorric dermatitis. Fungal infection of nail • Plaque • Guttate • Flexural psoriasis • Localised forms • Generalized pustular • Nail involment • erythroderma
plaque • Well defined,discoid plaques • Involves elbow,knees,scalp hair margin,sacrum • Plaques are red covered by waxy white scales which when removed leaves bleeding point known as ausptiz sign. • Plaques 2cm to several cm and may be itchy.
guttae • Acute ,symetrical eruption of drop like lesion • Commonly over the trunk and limbs • Most common in young adults • May follow a streptococcal throat infection.
flexural • Common sites are axillae,sub-mammary area and natal cleft, • Plaques are smooth and glazed. • Common in elderly.
Localized forms • Palmoplantarpustulosis • yellow to brown colored sterile pustules on palm and soles. • common in middle age females • Common in ciggarete smokers. • Scalp psoriasis: Can be confused with dandruff but are better demarcated and more thickly scaled. • Napkin psoriasis: • seen in infant in the nappy area • Lesion are well defined psoriasiform eruption are seen.
Generalized pustular • Rare but life threatening • Sheets of small sterile yellowish pustules appear on erythematous background and spreads rapidly • Acute onset • Fever , malaise and pt.requires hospital admission.
The skin initially becomes fiery red and tender. • Constitutional signs and symptoms, such as headache, fever, chills, arthralgia, malaise, anorexia, and nausea is present. • Within hours, clusters of nonfollicular, superficial 2 to 3mm pustules may appear. • The most common sites of involvement are the flexural and anogenital areas. Less often, facial lesions may also occur. • Pustules may occur on the tongue and subungually, resulting in dysphasia and nail shedding respectively.
These pustules coalesce within 1 day to form flakes of pus that dry and desquamate in sheets • Smooth erythematous surface is left on which new crops of pustules appear. • These episodes of pustulation may occur for days to weeks, thereby causing the patient severe discomfort and exhaustion. • A telogen effluvium type of hair loss may develop in 2-3 months. • Upon remission of the pustular component, most systemic symptoms disappear; however, the patient may be in an erythrodermic state or may have residual lesions of psoriasis vulgaris.
Other symptoms and signs • Fever • Dehydration • Itching • Weight loss • Muscle Weakness and fatigue • Fast heart rate • More severe complications may include breathing difficulties, low blood calcium levels, pneumonia, congestive heart failure and hepatitis. • Seeking immediate dermatologic care for this condition is important.
Causes The following have reportedly triggered an eruption: • Withdrawal of systemic steroids • Drugs like lithium, phenylbutazone, oxyphenbutazone, trazodone, penicillin, iodine, hydroxychloroquine, calcipotriol, interferon-alpha, and recombinant interferon-beta injection • Strong, irritating topicals, including tar, anthralin, steroids under occlusion, and zinc pyrithione in shampoo • Infections • Sunlight or phototherapy • Cholestatic jaundice • Hypocalcemia • Idiopathic in many patients
Treatment • Generalized pustular psoriasis is treated by: • Placing dressings soaked in a mixture of aluminum acetate and water over the affected areas. • Topical steroids may also be used. • Severe cases may require acitretin, methotrexate, or cyclosporine.
Nail involvement • Affects the nail matrix or nail bed • Commonest change ;thimble pitting followed by oncholysis(separation of distal edge of nail from nail bed) • Adjacent to onycholysis salmon pink discoloration is seen . • Subungal hyperkeratosis • Associated with psoriatic arthopathy.
Psoriatic arthropathy Occurs in about 5% cases. • Four forms: • Distal arthritis:Mostly causes swelling of interphalangeal joints of hand and feet,sometimes causing flexion deformity. Sausage like swelling of digits may occur. • Rheumatoid like arthritis:mimics rheumatoid arthropathy with polyarthopathy,but is less symmetrical and R.F factor is negative. • Mutilansarthritis:erosion develop in small bones of hand and feet,sometimes in the spine. The bones may be dissolved giving severe deformity. • Ankylosingspondylitits
Fixed flexion deformity of distal interphalangeal joints following arthropathy.
Rheumatoid-like changes associated with severepsoriasis of hands.
Erythrodermic psoriasis • Also known as generalised exfoliative dermatitis. • Any inflammatory dermatosis that involves all or nearly all skin surface.
pathophysiology • Acute • Chronic Acute form:Odema of epidermis and dermis is prominent and is inflitrated by inflammatory cells. Chronic form: There is lenghtening of rete ridges and thickening of epidermis.
causes • Eczema (40%) • Psoriasis(25%) • Lymphoma(15%) • Drug eruption(10%) • Pityriasis rubra pilaris(1%) • Unknown(8%)
Erythrodermic psoriasis may be precipitated by: • Infections • Low calcium • Withdrawal of oral corticosteroids (prednisone) • Withdrawal of excessive use of strong topical corticosteroids • Strong coal tar preparations • Certain medications including lithium, antimalarials
It is a dermatological emergency • Common in male and middle aged and elderly. • Often developd suddenly especially when associated with leukemia or eczema. • A patchy erythema develops which spreads all over the body within 12-48 hours and accompanied by pyrexia ,malaise,shivering . • After 2-6 days scaling appears and the skin appears hot, red dry and thickened. • The exfoliation of skin is continous and copious.scalp and body hair is lost .nail become thickened and is shed. • Pigmentary changes occur and those with a dark skin hypopigmentaion is seen.
complications • Cardiac failure • Hypothermia:failure to sweat and excess heat loss. • Dehydration • Hypoalbuminaemia:protein loss in exfoliated scales. • Cutaneous oedema:hypoalbuminaemia.
Management • Inpatient treatment essential . • Nursed in a warm room at a steady temperature.(30-32degree) • Pulse,BP,temperature and fluid balance should be monitored regularly. • Tropical steroid and bland cream are main stay of treatment. • Systemic steroid are life saving in emergency cases.
Treatment of psoriasis • Explanations and reassurances must be given to the patients or the parents. • Information leaflets help to reinforce verbal advice. • At present there is no cure for psoriasis; all treatments are suppressive and aimed at either inducing a remission or making the condition more tolerable. However, spontaneous remissions will occur in 50% of patients.
Local Therapies • Topical Corticosteroids • Topical Vitamin D3 Analogues • Topical Retinoids • Photo(chemo)therapy Systemic Therapies • Oral • Parenteral
Topical corticosteroids • High potency and Super potent topical steroids • These include • Fluocinonide (cream, ointment, gel) • Betamethasone dipropionate cream • Clobetasol propionate (cream, ointment, gel, foam, lotion) • Diflorasone diacetate ointment • Betamethasone dipropionate ointment
Topical corticosteroids • Side effects associated with use • Skin atrophy • Burning and stinging • Suppression of the hypothalamic-pituitary-adrenal (HPA) axis • This may occur after 2 weeks of use with certain topical corticosteroids
Topical Vitamin D3 Analogues • Prototype for this group is calcipotriene • 3 formulations – cream, ointment, and scalp solution • Former two are approved for plaque psoriasis • Latter for moderate to severe psoriasis of the scalp Topical Vitamin D3 Analogues • Side effects associated with use • Cutaneous • Burning • Stinging • Pruritis • Skin irritation • Tingling of the skin
Ultraviolet B (UVB) • Treatment is time consuming • 2-3 visits/week for several months • Side effect – possibility of experiencing an acute sunburn reaction
Photo(chemo)therapy • Two types of phototherapy • Ultraviolet B (UVB) • Ultraviolet A + psoralen (PUVA)
PUVA • Consists of ingestion or topical treatment with a psoralen followed by UVA • Usually reserved for severe, disabling psoriasis • Time consuming – 2-3 visits/wk; at least 6 weeks • Precautions • Patients must be protected from further UV light for 24 hours post treatment • Side effects with oral psoralen • Nausea • Dizziness • Headache • Side effects with PUVA • Early • Pruritus • Late • Skin damage • Increased risk for skin cancer, particularly squamous cell (SCC) and after 200 - 250 treatments, increased risk for melanoma
Systemic Therapies • Oral • Methotrexate • Cyclosporine • Oral retinoids (acitretin) • Parenteral • Amevive (alefacept) • Raptiva (efalizimab) • Enbrel (etanercept)
Methotrexate:Folic acid antagonist • Usually reserved for severe, recalcitrant, disabling psoriasis • Maximum improvement can be expected after 8 -12 weeks Side effects: • Acute or chronic hepatotoxicity • Hepatic cirrhosis • Leukopenia • Thrombocytopenia • Anemia, including aplastic anemia • Rarely, interstitial pneumonitis • Stomatitis • Nausea/vomiting • Alopecia • Photosensitivity • Burning of skin lesions