Download
1 / 24
250 likes | 262 Views
Explore the importance of patient self-management in chronic conditions like HIV, with evidence-based strategies for empowering patients and supporting healthcare providers. Learn about effective self-management tools and skills for improved outcomes.

E N D
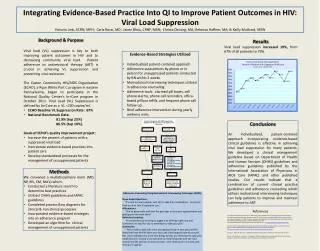
HIV Patient Self-ManagementThe Rationale, Evidence Base, and Practice Implications Joseph Rukeyser, PhD National Quality Center
Growing confidence in patient self-management “Increasing evidence shows that self-management support reduces hospitalizations, emergency department use, and overall managed care costs.” “Physician support of patient self-management is one of the key elements of a system’s-oriented chronic care model.” Coleman and Newton. Supporting self-management in patients with chronic illness. Am Fam Physician 2005;72(8):1503-10
Patient self-management is… “The ability of patients with chronic illnesses, in a complementary partnership with their health care providers, to manage the symptoms, treatment, lifestyle behavior changes, and the many physical and psycho-social challenges that they face each day.” A composite of definitions in the literature
HIV/AIDS as a chronic illness • Potent ARTs have transformed HIV into a chronic manageable disease • Many similarities to other chronic diseases but also important differences (stigma, drug resistance) • HIV therapy is life long • Treatment strategies must be sustainable • HIV patients have day-to day responsibilities for their care • Providers must support motivation, tools, and skills Aberg J. The Changing Face of HIV Care: Common Things Really Are Common. Ann Intern Med. 2006;145(6):463-65
Patient self-management is used effectively in chronic illnesses • Asthma “Educational programmes for the self management of asthma in children and adolescents improve lung function and feelings of self control, reduce absenteeism from school, number of days with restricted activity, number of visits to an emergency department, and possibly number of disturbed nights. Educational programmes should be considered a part of the routine care of young people with asthma.” Guevarra P et al.Effects of educational interventions for self management of asthma in children and adolescents: a systematic review and meta-analysis. BMJ 2003;326:1308-13
Patient self-management is used effectively in chronic illnesses • Diabetes • Group visits and individualized problem- solving based upon the empowerment model are effective self-management tools • Interventions result in • Improved recommended prevention behaviors • Improved health status (SF-36) • Fewer specialty and ED visits • Enhanced patient satisfaction and self-efficacy • Improved HbA1c levels Wagner E et al. Chronic care clinics for diabetes in primary care. Diabetes Care 2001;25:695-700 Anderson R et al. Patient empowerment: results of randomized controlled trial. Diabetes Care 1995;18(7):943-949
Patient self-management is used effectively in chronic illnesses • Osteoarthritis • “The self-management of arthritis programme reduced anxiety and depression and improved participants’ perceived self-efficacy to manage symptoms.” Buszewicz M et al. Self management of arthritis in primary care: randomised controlled trial. BMJ 2006;Online First bmj.com
Patient self-management skills • Effective patient self-managers: • Learn about their HIV disease • Develop effective communication skills • Actively partner with providers in decision-making • Practice action-planning and problem solving • Self-monitor symptoms and follow treatment directions • Seek expert medical care and advice • Use family, peer, and community support resources • Maintain emotional and psychological balance • Practice health-enhancing behaviors
Supporting patients in self-management… • recognizes the reality of patient responsibility for the majority of decisions and behaviors that affect their health • respects and supports patient autonomy, affirming provider responsibility “to” and not “for” patients • acknowledges that effective medical management requires collaboration between providers and patients
The physician’s role in supporting patient self-management “Physicians who want to provide increased support of their patients’ self-management are advised to address three areas: • structuring patient-physician interactions to include goal-setting and problem-solving strategies, • making office system changes, and • providing self-management education by linking patients to community self-management programs.” Coleman M. and Newton K. Supporting Self-management in Patients with Chronic Illness. Am Fam Physician. 2005;72;8:1503-10.
The physician’s role in supporting patient self-management • What advice and materials can we provide to patients to use in improving their self-management? • What do we need to help us help patients? • What system supports will help both providers and patients?
Sample self-management supports • Patient education classes, resource referrals and reading • Aids for action-planning, information organization, and decision-making • Two-way communication, information sharing, and resource development • Help in collaborative goal-setting, action-planning, and problem solving • System supports (group visits; reminder calls; pre-MD visit, medication guides, provider team coordination) • Clinical symptoms and side-effects self-monitoring guide • Ongoing assessment and adjustment to changing circumstances and behavior-change needs
Growing evidence that supporting patient self-management… • reduces hospitalizations • reduces ER visits • reduces overall managed care costs • increases patient satisfaction with care • improves health outcomes • Glycemic control • Nocturnal asthma symptoms • Blood pressure control Coleman and Newton, Am Fam Physician, 2005
Patient self-management education is one type of support “We found that patient use of CDSMP [*] was associated with better outcomes in all study domains- small but statistically significant improvements in health status, health behavior, and self-efficacy and less use of the ED.” *The Chronic Disease Self-management Program (CDSMP) is the model for classroom-based patient self-management education. It combines peer-led disease-specific education with training in communication skills, decision-making, action-planning, and health-promotion techniques. Lorig K, et al. Effect of a self-management program on patients with chronic disease. Eff Clin Pract. 2001;4:256-262.
Limitations of patient self-management education “While self-management education programs are conceptually appealing, and while there has been growing interest in them as a means of empowering patients, improving outcomes, and reducing health care costs, the findings of this review suggest that not all self-management education programs for all diseases are effective.” In a meta-analysis of 71 trials of self-management education across several chronic disease states: • “Patient self-management programs which tailor educational content and methodology to individual patients and which are integrated into medical care may prove to be more effective than structured self-management education courses, for which only specific patient subgroups may be ready.” Warsi A, et al. Self-management Education Programs in Chronic Disease. Arch Inter Med. 2004;164:1641-1649.
Self-management support goes beyond patient education • “Self-management is an essential part of chronic disease care, and it includes both patient and provider responsibilities. It is important that our thinking not be limited to its structured patient-education component alone. Interventions that combine various forms of patient education with physician facilitation of collaborative goal-setting are more likely to be successful.” Rukeyser J, Steinbock C, Agins, B. Self-management in Chronic Disease. JAMA. 2003;289(12):1508-9.
Provider-patient relationship is a key to patient self-management • “Findings from this study suggest that HIV-positive women who exhibit empowered behaviours received more information from their providers and reported better patient-provider communications. Thus, it is our recommendation that providers help cultivate such empowered behaviours in their HIV-positive female patients, and move toward developing treatment partnerships with their patients.” Marelich W and Murphy D. Effects of Empowerment Among HIV-Positive Women on the Patient-Provider Relationship. AIDS Care. 2003;15(4):175-181.
Few self-management studies in HIV patients • No strong evidence yet of efficacy • Only pilot studies have been done • Increase in self efficacy correlated with increase in CD4 count and decrease in viral load* • More studies needed of in-office interventions and system supports *Ironson G, Weiss S et al(2005) The impact of improved self-efficacy on HIV viral load and distress in culturally diverse women living with AIDS: the SMART/EST Women’s Project. AIDS Care 17:222-36
Stanford HIV Pilot Study • Pilot test of a seven-session group self-management course for HIV/AIDS patients • symptom severity index decreased in the education session group and increased in the control group. • Self-efficacy improved in the educational group and decreased in the control group. • Other secondary outcome measures (pain fatigue, psychosocial symptoms, changes in stress/relaxation exercises, and HIV/AIDS knowledge were not significantly different in the two groups. • No follow-up of this pilot study reported to date. • Patient education training manual: Living Well with HIV and AIDS by Gifford, Lorig, Laurent, and Gonzalez Gifford A, Pilot Randomized Trial of Education to Improve Self-Management Skills of Men with Symptomatic HIV/AIDS. JAIDSHR. 1998;18136-144.
HRSA HIV/AIDS advisory • “The incorporation of self-management education into CARE Act activities could empower patients to take a more proactive role in managing their illness and improving their quality of life. Moreover, HIV/AIDS self-management programs have the potential to serve as the foundation for a more effective and satisfying patient-provider partnership, to enhance the psychosocial and physical health of PLWHA, and reduce the resources needed for case management.” • HRSA supports the development and implementation of patient self-management initiatives for PLWHA in CARE Act funded programs HRSA CARE ACTION Newsletter Jan 2006
Barriers to initiating patient self-management support programs • Comfort with traditional model of care • Reluctance to lose “control” • Time constraints • Unpreparedness for dealing with “non-medical” issues • Reimbursement concerns • Lack of skills training • Insufficient support from management • Unfamiliarity with the evidence basis
Getting past the barriers • Join efforts with other self-management supporters • Use inservices and study groups to get “buy-in” from clinicians and administration • Create multi-disciplinary teams to plan and implement programs • Share the responsibilities of patient support among members of the health care team • Use community resources
Selected references Anderson R. Patient Empowerment and the Traditional Medical Model. Diabetes Care. 1995;18(3):412-5. Bodenheimer T, Lorig K, Holman H, et al. Patient Self-management of Chronic Disease in Primary Care. JAMA.2002;288(19):2463-2475. Coleman M and Newton K. Supporting Self-management in Patients with Chronic Illness. Am Fam Physician 2005;72:1503-10. Glasgow R, Davis C, Funnell M, et al. Implementing practical interventions to support chronic illness self-management. Jt Comm J Qual Saf. 2003;29(11):563-74. Gifford A, Laurent D, Gonzales V, et al. Pilot Randomized Trial of Education to Improve Self-Management Skills of Men with Symptomatic HIV/AIDS. JAIDSHR. 1998;18:136-144. HRSA HIV AIDS Bureau. Self-Management and the Chronic Care Model. HRSA CARE Action. January 2006. Warsi A, Wang P, LaValley M, et al. Self-management Education Programs in Chronic Disease. Arch Intern Med. 2004;164:1641-1649.
National Quality Center (NQC) 888-NQC-QI-TA NationalQualityCenter.org NQCTA@health.state.ny.us