Download

1 / 20
200 likes | 233 Views
Learn about India's RNTCP, aiming to decrease TB-related mortality and morbidity, with high case detection and cure rates. Discover the comprehensive program structure and monitoring strategies.

E N D
Revised National TB Control Programme (RNTCP) Central TB Division Directorate General of Health Services Ministry of Health & Family Welfare Nirman Bhawan, New Delhi 110 011
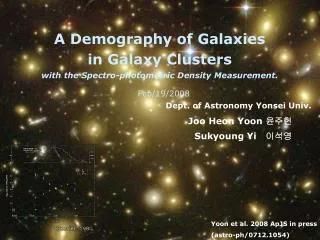
India is the highest TB burden country globally accounting for one fifth of the global incidence Global annual incidence = 8.9 million Source: WHO Geneva; WHO Report 2006: Global Tuberculosis Control; Surveillance, Planning and Financing
TB Burden in India Incidence of TB disease: 1.8 million new TB cases annually (0.8 million new infectious cases) Prevalence of TB disease: 3.8 million bacteriologically positive (2000) Deaths: about 370,000 deaths due to TB each year TB/HIV: ~2.5 million people with HIV; >1 million co-infected with HIV & TB About 5% of TB patients estimated to be HIV positive MDR-TB in new TB cases ≤3% and ~12% in Re-treatment cases Substantial socio- economic impact
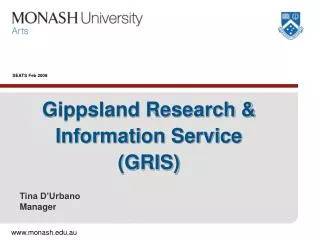
DOTS Coverage by District, India 31st March 2006 Nation wide DOTS coverage 632 districts – 1114 million people covered under RNTCP
RNTCP – Goal and Objectives Goal The goal of TB control Programme is to decrease mortality and morbidity due to TB and cut transmission of infection until TB ceases to be a major public health problem in India. Objectives: To achieve and maintain a case detection of at least 70% of new sputum positive TB patients To achieve and maintain a cure rate of at least 85% in such patients
RNTCP Performance National network of Diagnostic facilities 12,500 designated microscopy centres External quality assurance protocol in place Intermediate reference laboratories at State level for culture and drug sensitivity tests More than 8 million patients put on treatment NSP case detection rate for 3Q07 was 70% Treatment success rate maintained over 85% Death rate has fallen from 42/lakh pop (1990) to 29/lakh pop (2005)
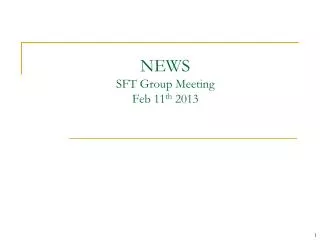
Annualized New Smear-Positive Case Detection Rate and Treatment Success Rate in DOTS Areas, India, 1999-2007* • Population projected from 2001 census • Estimated no. of NSP cases - 75/100,000 population per year (based on recent ARTI report)
Structure of RNTCP at State level STO, Deputy STO MO, Accountant, IEC Officer, SA, DEO State TB Cell Nodal point for TB control District TB Centre DTO, MO-DTC, LT, DEO, Driver One/ 5 lakh (2.5 lakh in hilly/ difficult/ tribal area) Tuberculosis Unit MO-TC STS, STLS One/ lakh (0.5 lakh in hilly/ difficult/ tribal area) MO, LT Microscopy Centre DOT Provider – MPW, NGO, PP, Comm Vol DOT Centre
RNTCP Laboratory Network 3 NRLs 24 IRLs ~12,000 DMCs (one per 50,000-100,000 population)
Lab Quality Assurance Senior TB Laboratory Supervisor (STLS) was provided to monitor quality of lab microscopy EQA protocol developed in 2001 In 2004, based on new international guidelines, External Quality Assessment (EQA) protocol was revised and implemented
Quality of treatment All patients initiated on treatment are monitored individually and treatment outcomes are reported through a system of cohort analysis DOT ensures that patients receive the right drugs in the right doses for the right duration of treatment All RNTCP patients receive drugs under direct observation by a accessible, acceptable and accountable DOT provider DOT provider may be health worker or community based volunteer, but not the family member
Patient-wise drug boxes A unique feature of RNTCP are the patient-wise drug boxes (for adult and paediatric cases), which improve patient care, adherence, and drug supply and drug stock management. Paediatric patient wise boxes introduced in 2006 M & E Monitoring through routine surveillance data, review meetings, Supervision at every level of programme Evaluation by the state, central level and 3 yearly joint monitoring missions All states are implementing the Supervision and Monitoring Strategy
Programme Surveillance System Peripheral Health Institute (DMC and other PHIs) Monthly PHI Report Tuberculosis Unit System electronic from district level upwards Quarterly CF, SC, RT, PM Reports Quarterly Feedback Additional Feedback District TB Centre Electronic reports) Quarterly Reports CF, SC, RT, PM State TB Cell Central TB Division
M & E Monitoring through routine surveillance data, review meetings, Supervision at every level of programme Evaluation by the state, central level and 3 yearly joint monitoring missions All states are implementing the Supervision and Monitoring Strategy
RNTCP “Supervision and Monitoring strategy” Strategy document developed and published in March 2005 All states and districts implementing the strategy All state/district programme staff trained in the strategy
RNTCP initiatives…1 DOTS Plus for MDR TB DOTS Plus services rolled out in Gujarat and Maharashtra in March 2007. Total of 74 patients put on DOTS Plus treatment. By 2010, programme plans to establish 24 DOTS Plus sites across the country Public private mix Over 2400 NGOs, 17,000 private practitioners and 120 corporate houses involved in RNTCP 246 Medical colleges involved and contributing 10-15% of case detection in their districts
RNTCP initiatives…2 TB HIV coordination National framework of joint TB HIV collaborative activities developed in 2007 Expansion of TB-HIV collaboration to all states will be done in 2008 6 fold increase in number of TB suspects referred from ICTCs to RNTCP since 2005 IEC (ACSM activities) Well defined communication strategy based on audience research and other aspects Web based IEC resource centre IEC baseline document has been developed in 2007 Communication facilitators appointed to support districts in planning and executing ACSM activities
RNTCP in NRHM State PIP In the NRHM “Programme Implementation Plan” (PIP), the states have to incorporate the various TB control activities and budget in Part ‘D’ of the PIP. The existing District Annual Action Plan/ State Annual Action Plan formats of RNTCP have to be incorporated in the NRHM State PIP.
ASHA for RNTCP The Accredited Social Health Activist (ASHA) - These community health volunteers have to be trained for DOT provision to provide affordable, accessible and quality treatment services near to patient’s home. These volunteers would be provided honorarium of Rs 250/- per patient on treatment completion.