Download
1 / 50
500 likes | 611 Views
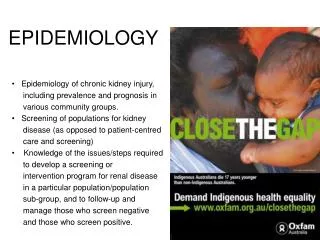
EPIDEMIOLOGY. By : dr. Siswanto , M.Sc. INTRODUCTION OF EPIDEMIOLOGY. Why does a disease develop in some people and not in others ? The disease and health problems are not randomly distributed in a population. DEFINITION.

E N D
EPIDEMIOLOGY By : dr. Siswanto, M.Sc.
Why does a disease develop in some people and not in others ?The disease and health problems are not randomly distributed in a population.
DEFINITION • The study of the distribution and determinants of health related states or events in specified populations, and the application of this to the control of health problems. • The study of the distribution and change in diseases. • The study of the distribution and determinants of disease in human population
“Study of disease and other health related phenomena in group of persons. (Kramer MS, 1988) • A science concerned with describing the pattern of disease occurrence in population and determining the factors which influence disease prevalence and distribution with the ultimate objective of providing the basis of control and prevention
The characterization of the distribution of health-related state or events is one broad aspect of epidemiology called descriptive epidemiology. • Epidemiology is also used to search for causes and other factors that influence the occurrence of health-related state or events. The latter is called analytic epidemiology
Descriptive epidemiology provides the What, Who, When and Where. WHATis the health problem , disease or event and what are its manifestations and characteristics ? WHOis affected with reference to age ,sex, social class, ethnic, occupation, heredity and personal habits ? WHENdoes it happen, in terms of days, months, seasons or years ? WHEREdoes the problem occur, in relation to place of residence, geographical distribution and place of exposure ?
Analytic epidemiology attempts to provide the Why, How and So What HOWdoes the health problem, disease or event occur, and what is its association with specific conditions, agents, vectors, sources of infection, susceptible groups and other contributing factors ? WHYdoes it occur, in terms of the reasons for its persistence or occurrence ? SO WHATinterventions have been implemented as a result of the information gained and what was their effectiveness ? Have there been any improvements in health status ?
What is hospital epidemiology? The fundamental roles of hospital epidemiology are to: • Identify problem • Identify risks • Understand risks • Eliminate or minimize risks
What questions Can be answered by Epidemiological Approach ? • How many peoples influenced by the disease? Since when the disease started, and do the number of cases tend to increase or decrease by time? • Do the disease burdened on a specific group of Age, gender, place, occupation, religion, economic status groups, marriage status, education? • What is the probable cause or risk factor that make the disease frequency? • Which of the cause / risk factors manageble? • What are the effective solution to control the disease ?
Case definition is a set of standard criteria for deciding a person has a particular disease (health related condition) or not
A Case definition consists of clinical criteria include : (symptoms/subjective complaints, signs/objective physical finding and laboratory test)
For example : in an outbreak of bloody diarrhea caused by infection with E coli O 157:H7, investigators defined cases in the following three classes : • Definite case : E coli O157:H7 isolated from a stool culture with gastrointestinal symptoms • Probable case : Bloody diarrhea with gastrointestinal symptoms • Possible case : Diarrhea and gastrointestinal symptoms
What kind of epidemiologicaltechnique needed in Community Diagnosis • The Disease Frequency measurement: • Prevalence and Incidence rate • Thetrends of Prevalence & Incidence • Thedistributionof prevalence or incidence rate by age, sex, occupation, socio-economic groups, place, religions • Formulate Hypothesisabout the risk factors (use la londe model) • Test hypothesis
SCHEME FOR AN EPIDEMIOLOGICAL STUDY CYCLE DESCRIPTIVE STUDIES ANALYSIS OF RESULTS, SUGGEST FURTHER-DESCRIPTIVE AND NEW HYPOTHESIS MODEL BUILDING FORMULATION OF HYPOTHESIS TEST HYPOTHESIS ANALYTICAL STUDIES EXPERIMENTAL STUDIES : - X - SECTIONAL - CASE-CONTROL STUDY - COHORT - CLINICAL TRIALS - FIELD TRIALS
RESEARCH DESIGN IN EPIDEMIOLOGY THE EPIDEMIOLOGY STUDY OBSERVATIONAL STUDIES (NO CONTROL OVER EXPOSURE) EXPERIMENTAL STUDIES (INFESTIGATOR DETERMINE) WHO EXPOSED OR NOT EXPOSED NO COMPARISON GROUP COMPARISAN GROUP DESCRIPTIVE ANALYTIC CROS SEC TIONAL STUDY CASE CON TROL STUDY COHORT STUDY CASE REVIEW SURVEILLANCE SURVEY
5 CRITERIA CAUSAL ASSOCIATION 1.TEMPORAL RELATIONSHIP --> means exposure to the causal factor (risk factor) must precede development of the disease (effect) 2. STRENGHT OF ASSOCIATION (RR> 4) --> Strength refers to the size/magnitude of RR (not the p value or degree of statistically significance which can be increased by increasing the sample size). 3. CONSISTENCY (C) AND REPLICATION (R) C--> means different studies resulted in the same association R--> means repetition of the same study resulted in the same association.
SPECIFICITY/DOSE-RESPONSE RELATIONSHIP Measures the degree to which one particular exposure produces one specific disease. • COHERENCE WITH EXISTING KNOWLEDGE (BIOLOGICAL PLAUSIBILITY) Support for the causal of an association exist if a causal interpretation is plausible in term of current knowledge about the factor and the disease.
PRINCIPLES OF CAUSALITY(SEVEN POINTS) • There should be evidence of a strong association between the risk factor and the disease ( Relative risk, odds ratio and prevalence ratio) • There should be evidence that exposure to the risk factor preceded the onset of disease • There should be a plausible biological explanation • The association should be supported by other investigations in different study setting
5. There should be evidence of reversibility of the effect. ( That is, if the “cause” is removed the “effect” should also disappear, or at least be less likely) 6. There should be evidence of a dose response effect.( That is, the greater the amount of exposure to the risk factor, the greater the chance of disease) 7. There should be no convincing alternative explanation. ( For instance, the association should not be explainable by confounding)
NATURAL HISTORY OF DISEASE Natural history of disease refers to the progress of a disease process in an individual over time, in the absence of intervention. The process begins with exposure to or accumulation of factors capable of causing disease. Without medical intervention, the process ends with recovery, disability, or death
NATURAL HISTORY OF DISEASE ONSET OF SYMPTOMS USUAL TIME OF DIAGNOSIS PATHOLOGIC CHANGES EXPOSURE SPECTRUM OF DISEASE STAGE OF SUSCEPTIBILITY STAGE OF SUBCLINICAL DISEASE STAGE OF CLINICAL DISEASE STAGE OF DISABILITY OR DEATH • RECOVERY • DISABILITY • DEATH WITHOUT MEDICAL INTERVENTION
NATURAL HISTORY OF DISEASE • For infectious disease, the exposure usually is microorganism. For infectious disease the period of subclinical is called the incubation period • For cancers, the critical factors may require both cancer initiators, such as asbestos fibers or components in tobacco smoke (for lung cancer) and cancer promoters, such as estrogens (for endometrial cancer). For chronic disease the period of subclinical is called the latency period
DISEASES CAUSATIONS • MOSTLY MULTIFACTORIALS (> 1 factor) • 2 THEORY : • EPIDEMIOLOGICAL TRIANGLE MODEL; • LA LONDE (Henry L Blum) MODEL.
EPIDEMIOLOGICAL TRIANGLE MODEL • The arising disease, is always a result of total interaction of 3 factors: • The Destructive power of AGENT OF DISEASE, as an absolute factor that must be exist as the cause. • The Defensive Power of HUMAN HOST as the target of agent of disease, and • The Supporting Power of the ENVIRONMENT to destructive power of agent of disease or to protective power of human host
DETERMINANT OF HEALTH EPIDEMIOLOGICAL TRIANGLE MODEL Resistance of Human host against disease Destructive power of Agent of diseases Environment
AGENT OF DISEASES • Physical agent: Temperature, dust, gas, light, noise, radiation, etc • Chemical Agent : Acid, Base, metal, Organic compound, food aditive, etc • Biological agent : Bactery, Insect, Allergen, Animal’s bites, etc • Intrinsic agent :Gen, hereditary disorders; • Psychologial agent : Mental Stress;
DESTRUCTIVE POWER OF AGENT OF DISEASE DETERMINED BY : • Quantity of agents; • Duration of contact with agent of disease; • Area of contact between agent of disease and body of human host; • Basic characteristic of agent of disease : Corosive, Allergen, Toxic, Carcinogenic, Mutagenic, Invasive, etc; • Tissue resistance of human host against agent of disease
HOST RESISTANCE • Host resistance against destructive power of agent of disease, determined by : • Genetic factors; • Mental & Spiritual stability • Nutritional status; • Physical fitness; • Immunity;
ENVIRONMENTAL FACTORS • EFFECT AGAINST AGENT OF DISEASE : • Increase /decrease number of agent of disease, duration of contact, area of contact and destructive power of agent of disease; • ex High air temperature lower the body indurance • EFFECT AGAINST HUMAN RESISTANCE : • Increase / decrease psicho-bio-physical indurance ; • ex Food production determine the nutritional status of population.
PSYCHO-BIOLOGICAL ENDURANCE HEALTH SERVICE PROGRAMS • ENVIRONMENT • Biological • Social LIFE STYLE DETERMINANT OF HEALTHLA LONDE MODEL Health problem
Threeterms are used to describe an infectious disease according to the various outcomes • Infectivity refers to the proportion of exposed persons who become infected. • Pathogenicity refers to the proportion of infected persons who develop clinical disease • Virulence refers to the proportion of persons with clinical who become severely or die
Chain of infection • Transmission of disease occur when the agent leaves its reservoir or host through a portal of exit, and is conveyed by some mode of transmission, and enters through an appropriate portal of entry to susceptible host. The process is called the chain of infection.
RESERVOIR • The reservoir of an agent is the habitat in which an infectious agent normally lives, grows and multiplies. • Reservoir include human, animal and the environment
Two type of human reservoir • Carrier is person without apparent disease who is capable of transmitting the agent to others. Asymptomatic carriers , who never show symptom during the time they are infected. Incubatory or convalescent carriers who are capable of transmission before or after they are clinical ill
Two type of human resevoir Chronic carriers is one who continues to harbor an agent for extended time (months or years). Exp : Hepatitis B, typhoid fever) • Symptomatic persons are usually less likely to transmit infection widely because their symptom increase their likelihood of being diagnosed and treated.
Portal of exit The path by which an agent leaves the source host. The portal of exit usually corresponds to the site at which the agent is localized. Examp : tubercle bacilli and influenza virus exit the respiratory tract, cholera vibrios in feces.
Modes of transmission • Direct Direct contact (kissing, sexual intercourse) Droplet spread ( refers to spray with relative large. Sneezing, coughing even talking) • Indirect ( an agent is carried from a reservoir to a susceptible host by suspended air particle, vector and vehicle) Airborne (The nuclei less than 5 μ/micron) Vehicleborne Vectorborne : Mechanical, Biologic
Portal of entry An agent enters a susceptible host through a portal of entry.
HEALTH • Health is a state of individual or community’s:physical, mental, spiritual, dan socialwellbeing and not merely a condition of free from illness and injury, so that every individual can achieve his/her social and economic productivity (Health Law No 23 th 1992). • Physical, mental, spiritual dan social component of health are inter-related one to each other, and create a health conditions of individuals or community. • The Integration of the 4 components of health, create an interval scale of health states or levels of health ranges from low health level to a perfect health level.
PHYSICAL MENTAL SOCIAL SPIRITUAL COMPONENTS OF HEALTHAND THE LEVEL OF HEALTH PERFECT STRUCTURE AND FUNCTIONS Perfect Health Worst STRUCTURAL & FUNCTIONAL DEFECTS
Consequences • Since the doctor’s main jobs are analysing whether her/his patients are healthy or not, meaning that they must conclude the existing conditions of the patient’s body & mind structure and/or function deviate from normality. • To be a skillfull doctors, the Medical Students must: • Have a good knowledge and skills in examining the structure and functions of normal and abnormal individuals (physically, mentally and socially); • Have a good knowledge and skills to stop the changing process of body structures and functions and then make it back to normal.
WHAT THE DOCTOR’S CANDIDATE MUST LEARN • The normal body and mind structure and functions (anatomy, histology, physiology, biochemistry) • Non-normal structure and functions (microbiology, parasitology, clinical pathology, anatomy pathology) • Laboratory and clinical skills to practice medical profession (Clinical Pre internship or Clerkship) • Management skills and knowledge of medical care services (Public Health) • Intelectual skills and knowledge (Methodology, Science Projects)
ILLNESS One’s perception on the signs of the deviations / abnormality of bio-psycho-socials structure or/and functions of their own or other’s Ex. Headache, Fever, pain, etc DISEASE One’s expectations upon causal factor/s that stimulate the structural and functional deviation of bio-psycho-social on their own or others Ex. HIV, Malaria, etc ILLNESS VS DISEASES
The Facts about Disease • Every disorder/diseases must be caused by at least one internal or external factors (mostly multifactors); • The degree of the disorders, depend on the destructive power of the causal factors, and the protective power of the individuals body and mentality. • There is always time lag (incubation period) between the exposure time of factors, and the development of sign or symptoms of diseases; • The prevention of diseases, is actually a process • to stop the worse development of diseases, as early as possible; • to normalize the structural and functional deviation to achieve the highest social and economic productivity.
USES • Population or community health assesment. To do this, we must find answers to many questions : What are the actual and potential health problems in the community ?, Where are they ?, Who is at risk ?, Which problems are declining over time ?, Which ones are increasing or have the potential to increase ?, How do these patterns relate to the level and distribution of services available ?. • Individual decisions. People may not realize that they use epidemiologic information in their daily decisions.
Completing the clinical picture. When studying a disease outbreak, epidemiologists depend on clinical physicians and laboratory scientists for the proper diagnosis of individual patients. But epidemiologist also contribute to physicians, understanding of the clinical picture and natural history of disease. • Search for causes. Much of epidemiologic research is devoted to a search for causes, factors which influence one,s risk of disease.
Health Status For example : Prevalence, Incidence • Evaluation of intervention. To assess the effectivenessof preventive and therapeutic treatments. To assess the impact of health-care services To predict future health care needs