Download
1 / 9
90 likes | 108 Views
Explore the revised evidence-based guidelines for diagnosing gout in rheumatology and primary care settings, incorporating clinical algorithms and imaging techniques. Aimed at healthcare providers managing gout patients.

E N D
2018 Updated EULAR Evidence-based Recommendations for the Diagnosis of Gout
Slide 1: Target population/question • In 2006, the EULAR produced its first evidence-based recommendations for the diagnosis of gout. Since then, a number of studies have explored the diagnostic value of clinical algorithms and of imaging modalities such as ultrasound (US) or dual-energy computed tomography (DECT). This prompted a revision of the 2006 recommendations following an updated systematic literature review (SLR) and a Delphi process to achieve consensus • Target population: Rheumatologists, GPs, and all Health care providers who manage people with Gout
Slide 2: Methods/methodological approach • Methods: According to the EULAR Standardized Operating Procedures* Consensual approach Systematic literature research Consensual approach FINAL Recommendations * van der Heijde et al Ann Rheum Dis 2016,75:3-15
Slides 3-4: Overarchingprinciples • Since we formulated only 8 recommendations, we did not propose overarching principles
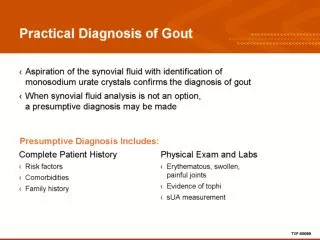
Slides 17-18: Summary of Recommendations in bullet point format • The task force recommends a three step approach for the diagnosis of gout • The first step relies on MSU crystal identification when SF analysis is feasible. • If not possible, the second step relies on a clinical diagnosis based on suggestive and associated clinical features of gout and presence of hyperuricemia. • When a clinical diagnosis of gout is uncertain and crystal identification is not possible, the third step recommends imaging, particularly ultrasound, to search for crystal deposits. • [Secretariat will add link of recommendation once available online on BMJ portal.]
Slides 19-20: Summary of Recommendations in lay format Read the full lay summary (add hyperlink if provided) 1 star (*) means it is a weak recommendation with limited scientific evidence; 2 stars (**) means it is a weak recommendation with some scientific evidence; 3 stars (***) means it is a strong recommendation with quite a lot of scientific evidence; 4 stars (****) means it is a strong recommendation supported with a lot of scientific evidence. Recommendations with just 1 or 2 stars are based mainly on expert opinion and not backed up by appropriate clinical studies, but may be as important as those with 3 and 4 stars.
Slide 21: Acknowledgements • This paper is dedicated to the memory of Dr Victoria Barskova. The task force thanks EULAR for financial and logistic support.